Next-generation sequencing (NGS) has been proposed as a suitable tool for liquid biopsy in colorectal cancer (CRC), although most studies to date have focused on sequencing panels of potential candidate genes that are clinically actionable 31. In our case, we tested a new approach called differential presence of exons (DPE) described by the Garcia-Olmo research group at the University Hospital Fundación Jiménez Díaz 17. This NGS approach at a relatively shallow depth represents an easy, rapid, non-invasive and affordable strategy for future use in clinical practice.
Mutation analysis by liquid biopsy presents several challenges; one of them is the sensitivity of DNA detection, which is affected by cfDNA concentration 32, background noise rate, ctDNA abundance in plasma, capture efficiency, and requires high sequencing depths for detection 33,34, in addition to tumor heterogeneity and the presence of variants caused by clonal hematopoiesis 35,36. Sometimes, detecting these mutations is difficult because the patients still have a small tumor mass, producing low ctDNA rates which results in a negative result. To solve this, high sequencing depths are required, being a costly strategy in expanded NGS panels.
This DPE approach has the advantage of avoiding these challenges. We have obtained significant results, quality of reads and optimal read depth. This supports the usefulness of DPE as a new technique to analyze cfDNA from cancer patients, specifically in CRC. However, there could be some factors that could influence cfDNA analysis results, such as the technique used, the genetic profile analyzed, tumoral stage or tumor heterogeneity degree.
Our objective was to evaluate the whole exome sequence, under the DPE approach, as a tool to identify a DPE signature that could identify differential profiles between CRC patients with disseminated disease compared to CRC patients with localized disease or healthy controls.The cfDNA analysis could come from both tumor and non-tumor DNA, assuming that the cfDNA from patients with metastatic CRC was enriched in ctDNA as previously described 37–39. This is the main reason, why most of the comparisons were with the metastatic group.
Previous studies from our own group identified a DPE signature between metastatic vs non-metastatic patients and examined the reproducibility of the predictive algorithm using DPE in a rat model of metastatic colon cancer 17,18. In this study we went further, using a more novel and robust technology, to draw a signature in common between the metastatic vs non-metastatic, cancer group vs healthy control and metastatic vs healthy control comparisons, with the aim of discriminating between them, describing a DPE signature.
Through the M and N comparisons we were able to define differential 1,760 exon set, some overrepressed in the metastatic group and others in the non-metastatic group. The same for the cancer group vs healthy control and metastatic vs healthy control comparisons. It was seen that there were 510 exons in common between these comparisons that could explain the overall variation.
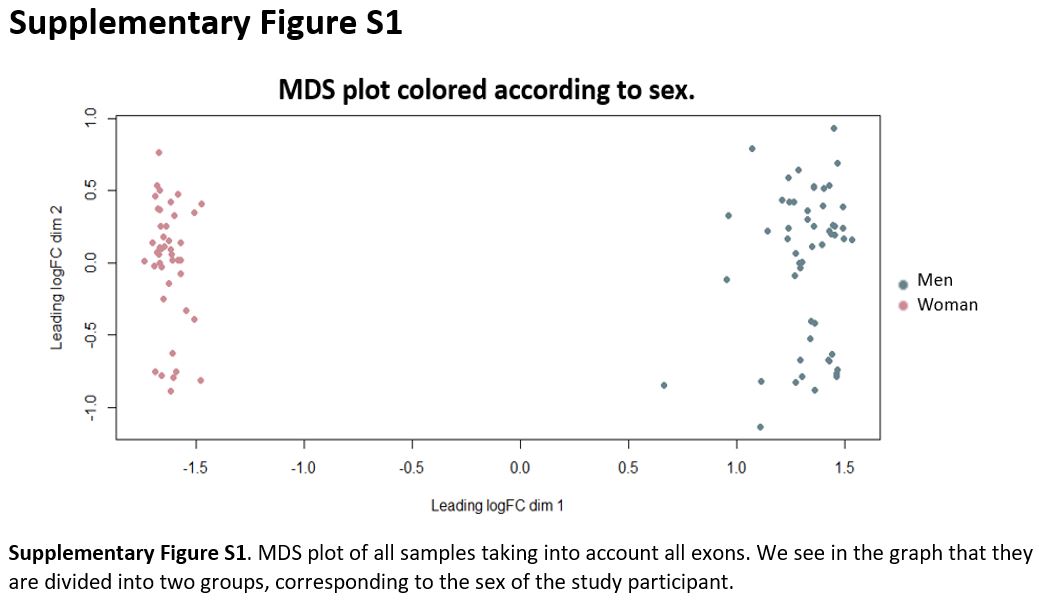
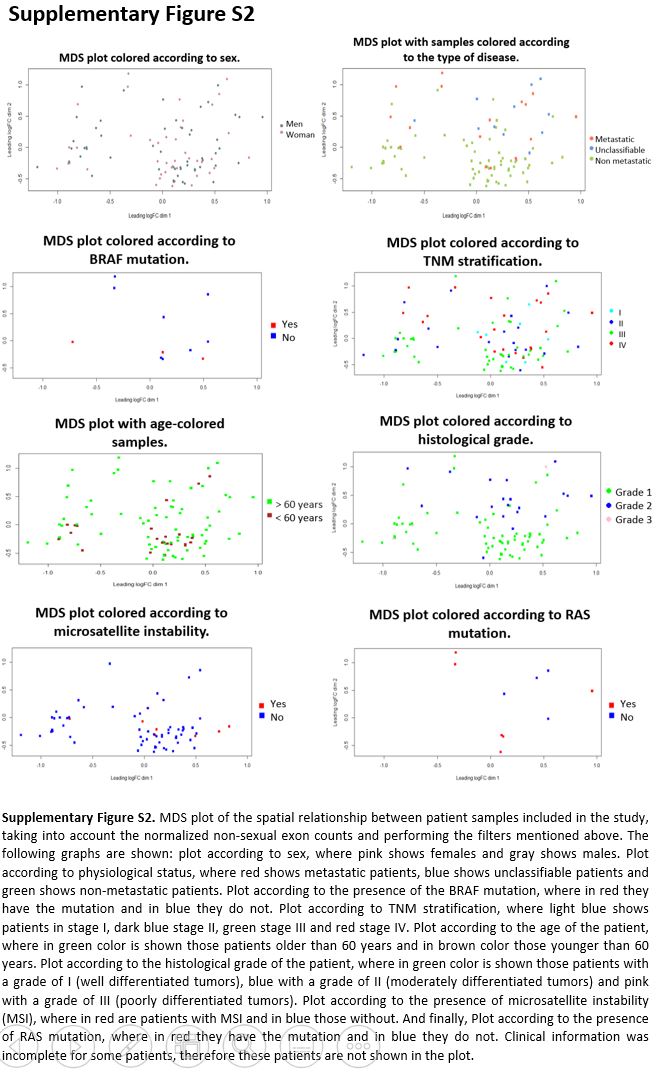
The resulting common DPE profile was used to cluster and classify all study participants and this information was processed to develop a DPE algorithm generating a predictive model using machine learning. Most patients were correctly grouped and separated between metastatic and non-metastatic, and it was also observed that when using these 510 DPEs healthy controls were placed in a point cloud in the PCA. Unclassifiable patients were clustered between groups. It is worth noting that the random forest results, gave us an error of 35.9% and with the data test, the model gave us an accuracy of 75% with 95% CI 56.6–88.5, with a sensitivity of classification of metastatic 20%, non-metastatic 83% and healthy 87%, with a specificity of 100%, 70% and 88% respectively.
These results encourage us to design further studies to confirm the predictive and prognostic value of our model, as well as to evaluate its usefulness for early identification of high-risk patients.
In another case, differential detection of exons suggests differential release of cfDNA actively by tumor and non-tumor cells, which could have biological implications by acting as a means of intercellular communication. Previous studies have described that cell-free nucleic acids circulating in the plasma of patients with colorectal cancer induce oncogenic transformation of cultured cells susceptible 40, and further that colorectal cancer cells can transfer the KRAS oncogene to distant cells, predisposing them to malignant transformation (genometastasis theory) 41. This makes us believe that this DPE signature could have some implication in malignant transformation.
It has been suggested that metastatic seeding may occur before clinical detection 42 and cfDNA may be involved in the metastatic process 43 and we suggest that one way to detect this could be from the DPE signature. Hence, NGS may be valuable, not only for clinical use, but also to gain insight into the highly complex mechanism of cancer progression.
Returning to the nature and the origin of these exons, we can say that they can be stably secreted into circulation and according to the Tape Station plots of the size distribution in nucleosomes, it is observed that these exons are released by apoptosis, as also shown in 44. The size distribution reflected two nucleosomes, which is common in liquid biopsy studies 45. These DPEs could be incorporated into microvesicles and exosomes to be protected from digestion enzymes 46–48. Recently DNA from exosome isolated from ascites of ovarian cancer patients has been described reflecting copy number variation in primary tumors 49,50 and in CRC, copy number alteration in KRAS in exosomes has been described that correlated with tumor size 51. Extracellular vesicles are increasingly becoming important mediators of intercellular communication. They play an important role in numerous physiological and pathological processes, and show great promise as novel biomarkers of disease 52. Specifically, it would be interesting to discover whether these DPEs could propagate signals intercellularly and cause deleterious effects at a distance.
These observations are critically important because they shed light on the intercellular role of cfDNA as signaling mediators and therapeutic strategies could be developed.
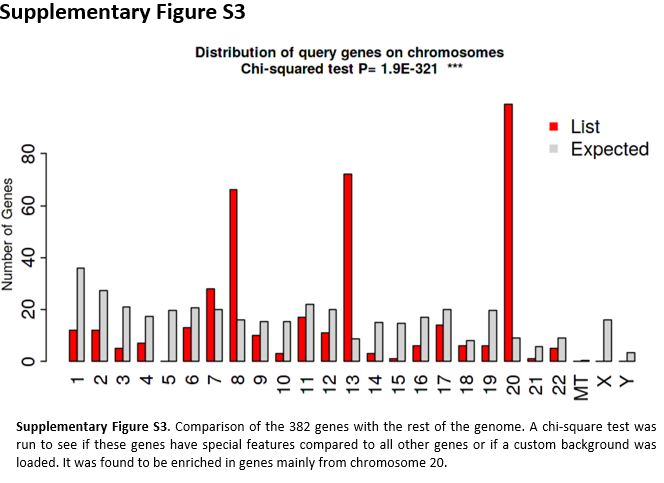
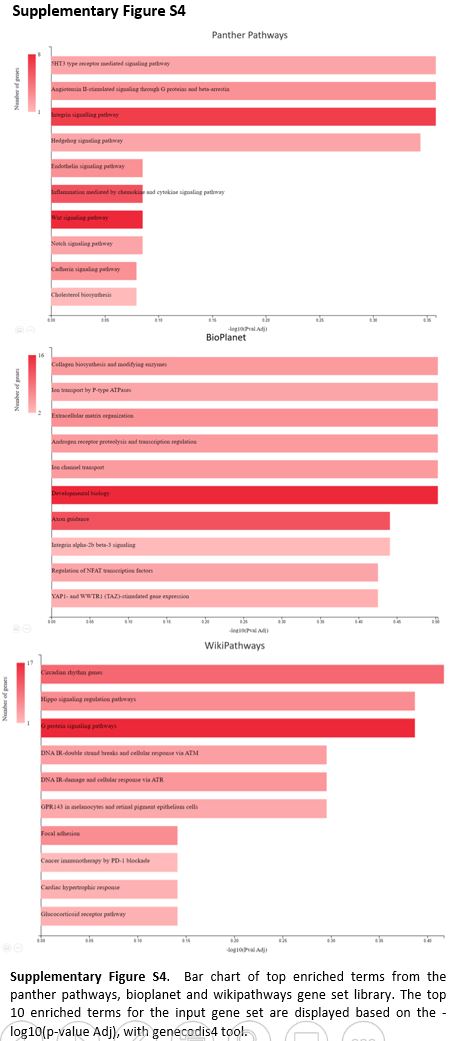
When performing the functional analysis of the 510 DPEs, we observed significant results in cancer related pathways such as; kidney cancer, where association with CRC has been described 53 and liver cancer, where we know that most CRC metastases occur in the liver 54. Therefore, this 510 DPE’s signature is enriched in exons from genes involved in cancer-associated pathways. In addition, we found trends in pathways such as estrogen signaling and it has been described that cancer cells induce the synthesis of more E2 to meet tumor needs by regulating key enzymes involved in the biosynthesis of these hormones 55 and has been associated with CRC 56.
The results obtained with Gene Ontology have also been associated with colorectal cancer in different research articles such as GO:0005021 (vascular endothelial growth factor receptor activity) 57 and GO:0032720 (negative regulation of tumor necrosis factor production) 58. This trend towards these pathways should be validated in the future.
DPE discovery not only may contributes to elucidating the molecular mechanism of carcinogenesis, but also provides a new approach to liquid biopsy analysis and proposes the use of DPE as a non-invasive biomarker. It is noteworthy that our study was original, and stands out against previous studies, which mainly focus on genetic alterations related to cancer.
The strengths of our study are that we have increased the number of study participants, we have included healthy controls that we were not included in previous studies. We have also innovated in the use of new exome technology, as well as a implemented a new standardized cfDNA extraction protocol that could facilitate its incorporation into clinical practice. In the future, we would consider using Agilent's BRAVO equipment to automate the library preparation process to avoid any human bias. Despite the results obtained, we must keep in mind the limitations of our study; because the fold-change difference is very low, we need to increase the number of samples in our study to have more conclusive results.
To conclude, it should be commented that liquid biopsy analysis can be used to gain new insights into the biology of metastasis and as a companion diagnostic to improve the stratification of therapies and to obtain information on therapy-induced cancer cell selection (precision medicine) and the technical and clinical validation of assays is very important 59.
{kind=link}
{kind=link}
{kind=link}
{kind=link}