Patient selection and data collection
To evaluate and validate the potential risk factors associated with NAC ischemia necrosis, patients who underwent NSM from January 2011 to September 2021 were retrospectively identified from a prospectively maintained breast cancer database at Changhua Christian Hospital (CCH), a tertiary medical center in central Taiwan. Those patients whose clinicopathologic factors, or information regarding the types of skin incision, post-operative NAC or skin flap ischemia necrosis status could not be clearly identified were excluded.
The collected data was obtained from the medical records of these patients, including age, BMI, pathologic reports, complications, ischemia necrosis of the NAC or skin flap, the location of the surgical incision, and status of follow-up. Patients with pre-operative breast MRI were further analyzed with pattern of blood supply (single vessel or double vessel) of the breast, and the diameter of the vessel. The pattern of blood supply and diameter of blood vessel was correlated to ischemia necrosis of NAC or skin flap condition to determine whether this information was predictive of NAC or skin flap necrosis. We also combined blood supply pattern (single- versus double vessel) in different type of skin incisions to assess the role of blood supply pattern and impact on ischemia necrosis of NAC. A literature review of reported studies (11, 16, 17, 19, 21-31) regarding risk factors and incidence of NAC ischemia necrosis was also performed in current research.
According to the inclusion and exclusion criteria, a total of 441 NSM procedures were identified and enrolled in current study, and among them, 270 cases had pre-operative breast MRI, which enable further analysis of blood vessel type and diameter to the survival or ischemia necrosis of NAC. The study was approved by the Institutional Review Board of the CCH (CCH IRB No. 141224 & 201242), and all participating patients had signed the related informed consent. The study design and patients’ flow chart were shown in Fig 1.
Grading of nipple-areolar complex (NAC) ischemia and necrosis
In this study, nipple ischemia necrosis was divided into 4 levels, designated as grade 0, 1, 2, and 3 (Fig 2). In grade 0 NAC ischemia/necrosis, the nipple is normal, there is no necrosis of NAC at all. Grade 1 NAC ischemia/necrosis, NAC underwent transient ischemia injury with slightly gangrene change, which was reversible after conservative treatment. There would be minimal (<25%) to no volume loss of the nipple after recovery. Grade 2 NAC ischemia necrosis, which nipple underwent irreversible moderate ischemia necrosis, and eventually leading to loss of around 50% (25-75%) of the original volume. Grade 3 NAC ischemia necrosis is the most severe form of necrosis injury. The NAC suffered from nearly (>75%) to complete (100%) loss of volume and eventually leading to surgical excision or total loss of the NAC tissue.
To evaluate the risk factors associated with NAC ischemia necrosis, those patients who suffered from grade II or grade III NAC ischemia necrosis (Fig 2) were recorded as events of NAC necrosis in current study.
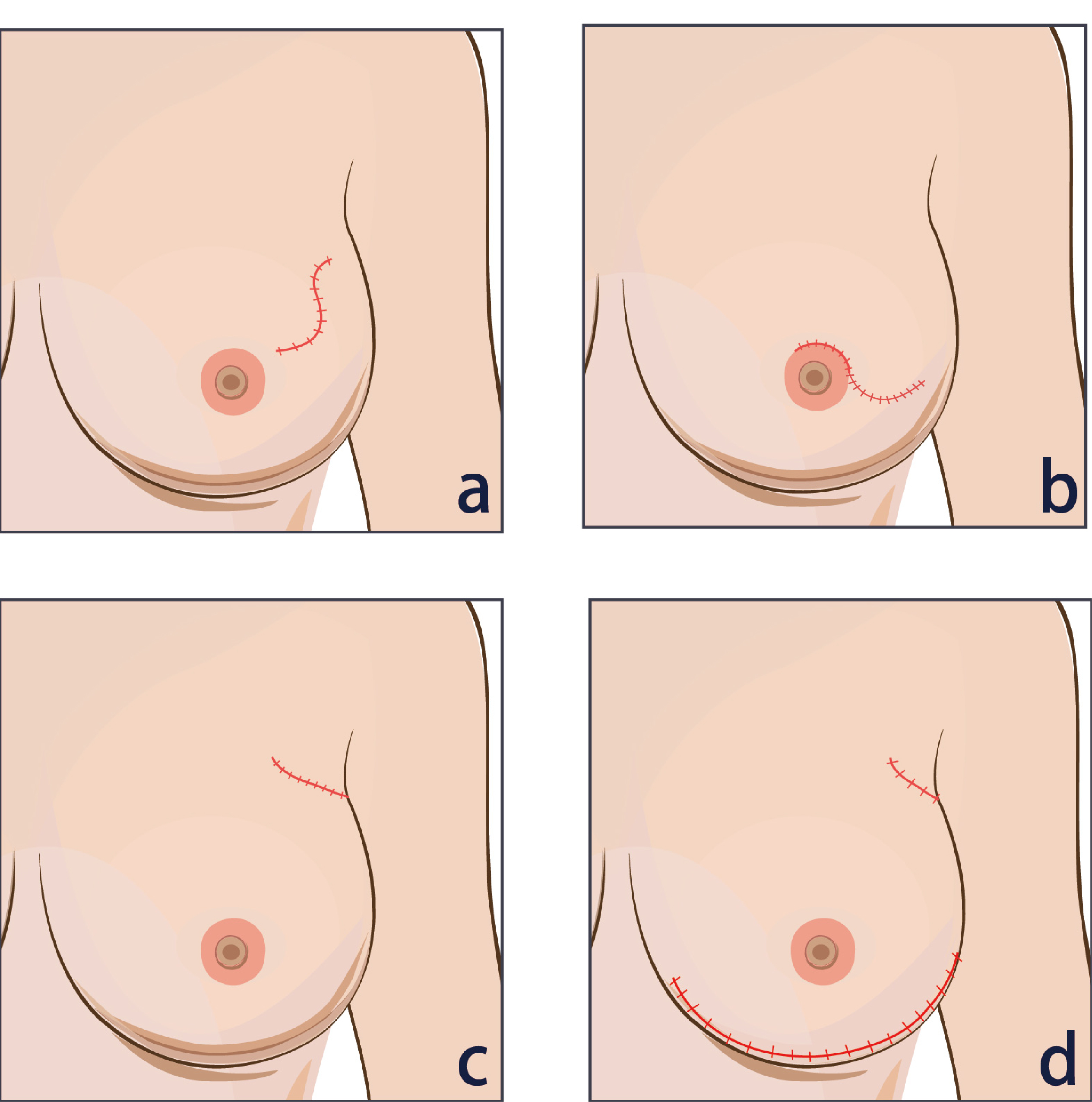
Type of skin flap incisions
Skin incisions were divided into the following categories for analytic purpose: upper outer incision (radial incision), peri-areolar incision (with or without axillary incision), single axillary incision, and infra-mammary +axillary incisions (Supplementary File 1). The NSM procedures performed with single axillary incisions in current study were mainly cases performed with endoscopic assisted or robotic assisted NSMs(32).
Body mass index (BMI) category
BMI was calculated as weight in kilograms divided by height in meters squared (BMI = kg/m2). Using Taiwanese definition, BMI was categorized into four groups: underweight (BMI <18.5), normal (BMI of 18.5 to 24), overweight (BMI of 24.1 to 26.9), and obese (BMI≥27). Patients were further categorized into 2 groups, which included non-obese (BMI <27) and obese (BMI ≥27), for analytic purpose in current study.
Magnetic Resonance Imaging (MRI) and protocol
MR imaging was performed with a Siemens MAGNETOM Verio 3.0 Tesla MRI machine. All patients were imaged in the prone position with both breasts placed into a dedicated 16-channel breast coil. MR imaging protocols included the following: bilateral axial turbo-spin-echo fat-suppressed T2-weighted imaging (TR/TE 4630/70 ms; field of view 320 mm; slice thickness 3 mm; number of excitations 1), axial turbo-spin-echo T1 weighted imaging (TR/TE 736/9.1 ms; field of view 320 mm; slice thickness 3 mm; number of excitations 1), and diffusion weighted imaging (TR/TE 5800/82 ms; field of view 360 mm; slice thickness 3 mm, with b-values of 0, 400, and 800 sec/mm2). Dynamic contrast enhanced MR images (DCE-MRI) were obtained with a three-dimensional fat-suppressed volumetric interpolated breath-hold examination (VIBE) sequence with parallel acquisition once before and five times after a bolus injection of gadobenate dimeglumine (0.1 mmol/kg). Both breasts were examined in the transverse plane at 60 s intervals in each phase of the dynamic studies. The dynamic MRI parameters were as follows: TR/TE 4.36/1.58 ms; field of view 320 mm; slice thickness 1 mm. The whole breast MRI readings were carried out by two experienced, board-certified breast radiologists (WPW and CYL).
Breast MRI had been part of pre-operative evaluation for breast cancer patients diagnosed and treated at CCH. Patients who underwent pre-operative breast MRI were retrospective evaluated with blood flow pattern. To understand the distribution and blood supply of blood vessels around the areola, MRI is used to assess the type of blood vessels around the areola. The blood supply is divided into dual blood supply and single blood supply. The diameter of the blood vessel was also divided into less than 1 mm, equal to 1 mm, and greater than 1 mm. The interpretation of blood vessel type and pattern was done by experienced breast imaging radiologist (WPW), who had more than 10 years’ experience in breast MRI.
Statistical analysis
Data are expressed as mean ± standard deviation, and compared using the parametric two-sample t-test. Baseline data was analyzed using chi-square tests (categorical data), or student's t test (continuous data). Associations between nipple ischemia necrosis and risk factors of patients were analyzed using the chi-square test. Multivariate logistic was performed to assess the association between NAC and/or skin flap ischemia necrosis and risk factors. Results were considered statistically significant if the two-tailed P value was <0.05 for all tests. Statistical analyzes were performed using SAS 9.4 version (SAS Inc., Cary, NC, USA) by statistic expert (YYL).
{kind=link}