3.1. Preparation, Characterizations and Rheology Properties of HA-EPL Coacervates
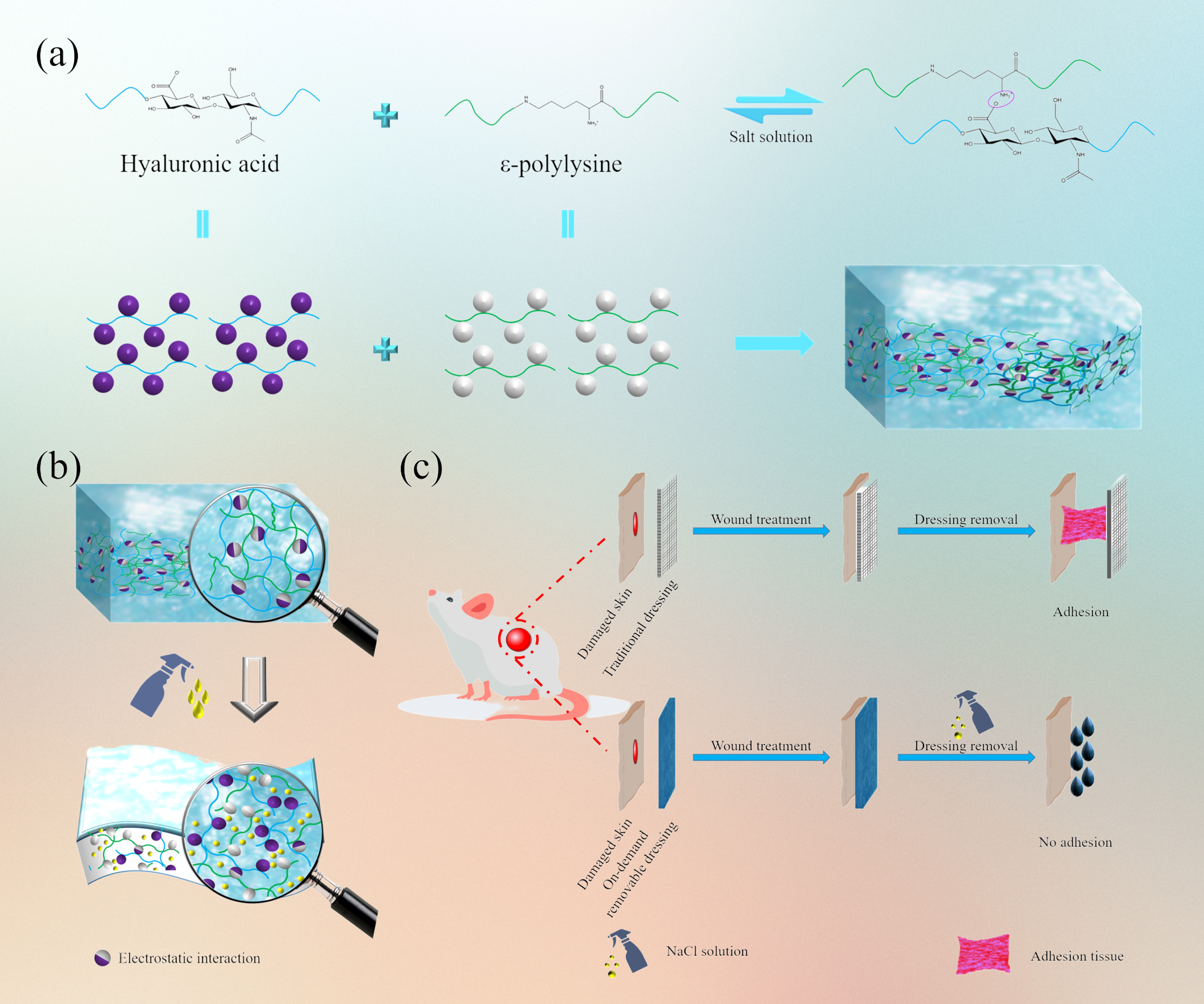
With a simple and feasible method, a new kind of injectable, self-healing, and on-demand removal dressing was successfully prepared. As revealed in Fig. 1a, after shaking and standing for 10 min, the mixture of HA solution and EPL solution completely separated into a light yellow coacervate phase and a corresponding supernatant. It could be observed that the coacervate droplets with sizes of several micrometers to tens of micrometers were dispersed in the aqueous environment (Fig. 1b), where large droplets consisted of small droplets[31]. SEM images of HA-EPL coacervates were shown in Fig. 1c. The pore diameter of 6% HA-EPL was close to that of 8% HA-EPL, while 4% HA-EPL showed a larger pore diameter and more extended size. This might be attributed to the insufficient number of amino groups and the weak electrostatic interactions in 4% HA-EPL[32]. Nevertheless, the presentation of the porous structure suggested that HA-EPL coacervates possessed the potential to be used as a dressing.
Electrostatic interactions and hydrogen bonds synergistically facilitated the formation of HA-EPL coacervates by FTIR analysis (Figure S1). In the spectrum of 8% HA-EPL (HA-EPL coacervates with EPL concentrations of 4%, 6%, and 8% were named as 4% HA-EPL, 6% HA-EPL, and 8% HA-EPL.), peaks at 1413 cm− 1 and 1618 cm− 1 which were related to the stretching vibration of the carboxylic group weakened or disappeared because HA was involved in the formation of HA-EPL coacervates. Besides, a decrease in the intensity of bands associated with amide Ⅰ, Ⅱ, and Ⅲ (1674 cm-1, 1564 cm-1, and 1255 cm-1) was also observed. This change might be attributed to electrostatic interactions between the amino groups of EPL and the carboxyl groups of HA during the formation of HA-EPL coacervates[32]. In addition to electrostatic interactions, the O-H stretching band in HA (3405cm-1) and the N-H stretching band in EPL (3419 cm-1) were shifted to 3431cm-1, meaning that hydrogen bonds formed in the formation process of HA-EPL coacervates[33].
The viscoelastic behaviors of HA-EPL coacervates were determined to further investigate their mechanical properties. In strain sweep tests (Fig. 1d), the values of G' and G" for HA-EPL coacervates prepared by different ratios were assessed. HA-EPL coacervates had a linear viscoelastic region and values of G" > G' when the strain ranged from 0.1–10%. In the time sweep tests (Fig. 1e), the values of G" were always higher than G' for 6% and 8% HA-EPL and no intersection was observed during the test time (0–5 min). However, for 4% HA-EPL, the G' and G" values marginally increased and finally intersected over time, thus indicating that the network structure of 4% HA-EPL was disturbed and better stability was achieved with 6% and 8% HA-EPL. In the frequency sweep tests (Fig. 1f), G' and G" values for 4%, 6%, and 8% HA-EPL gradually increased within the test frequency of 0.1–35 Hz. Besides, G" > G' of 4%, 6%, and 8% HA-EPL were observed when frequencies were 4.5, 6.0, and 10.8 Hz, respectively. This further
indicated that the stability of 8% HA-EPL was better than 4% and 6% HA-EPL. Besides, dressings with the injectable property have various advantages such as ease of operation and matching with the wound perfectly (Figure S3)[34]. As shown in Fig. 1g, the viscosity of 4%, 6% and 8% HA-EPL significantly decreased with the increase of shear rate, suggesting that HA-EPL coacervates exhibited a typical shear-thinning behavior and the preferable injectability. Also, HA-EPL coacervates could be continuously extruded from the needle (Movie S1) and draw letters of “XJTU” without clogging (Figure S4). The above results demonstrated that 8% HA-EPL with the preferable injectability, which could maintain a stable state for a long time, possesses potential as a medical dressing.
3.2. Self-Healing, Tissue-Adhesive and On-demand Removal Properties of HA-EPL Coacervates
Excellent self-healing ability enabled HA-EPL coacervates to cope with various accidental dressing damage. Thus, the self-healing ability of HA-EPL coacervates was determined by the step-strain-sweep scanning test. The G' and G" values of 4%, 6%, and 8% HA-EPL returned to original levels when the strain was converted between 0.5% and 500% (Fig. 2a), indicating that the collapsed structure of HA-EPL coacervates could rapidly recover. Besides, this collapse-recovery process could be repeated at least four times, demonstrating that HA-EPL coacervates possess efficient and rapid self-healing ability. Macroscopically, two separate heart-shaped 8% HA-EPL patches could heal rapidly in 30 seconds with almost no cut section, further confirming the excellent self-healing ability of HA-EPL coacervates (Fig. 2b).
Good adhesion ensures that the dressing is stably anchored to the skin to protect the wound. As shown in Figure S5, an 8% HA-EPL patch adhered firmly to the surface of porcine skin and even stuck two separate pieces of porcine skin together very well. Besides, the 8% HA-EPL patch exhibited satisfying adhesiveness to mice organs (Fig. 2d). This good adhesion performance was mostly attributed to the residual amino groups and carboxyl groups on the surface of HA-EPL coacervates, contributing to HA-EPL coacervates binding on the skin surface[35].
Traditional dressings often cause pain when they were peeled from injured skin. Besides, current dressings deliberately emphasize their excellent tissue adhesion, while the replacement of dressings has not been discussed in detail. On-demand removal dressings could reduce patients' distress due to adjustable adhesion. Thus, given the ability of the salt solution to weaken the electrostatic interactions between HA and EPL, HA-EPL coacervates were predicted to be sensitive to NaCl solution. As expected, 4%, 6%, and 8% HA-EPL partially dissolved within 30 min when immersed in different NaCl solution concentrations. Subsequently, 4%, 6%, and 8% HA-EPL were no longer observed after soaking in NaCl solution for 2 h (Figure S6). SEM images revealed that 4%, 6%, and 8% HA-EPL displayed a porous structure, while this porous morphology became irregular after 1 M NaCl solution treatment, indicative of the NaCl solution-induced destruction of HA-EPL coacervates’ network (Fig. 3a). Furthermore, rheological tests were performed to investigate the dissolution behavior of HA-EPL coacervates. As revealed in Fig. 3b-d, when exposed to 0.5 M NaCl solution for 20 min, the G" of the 4%, 6%, and 8% HA-EPL showed a modest decrease. Following on, the G" of the 4%, 6% and 8% HA-EPL showed a substantial decrease if 4%, 6% and 8% HA-EPL were immersed in 1 and 2 M NaCl solutions. Predictably, HA-EPL coacervates could be effectively removed when adhering to the wound. As presented in Fig. 3e, 8% HA-EPL was injected onto a rat wound, after which the gauze, infiltrated with 1 M NaCl solution, was gently placed on the 8% HA-EPL. After 20 min incubation, nearly all of the 8% HA-EPL covered by the NaCl-soaked gauze dissolved (Movie S2). Besides, the process of on-demand removal on the human hand was shown in Movie S3.
3.3. Antibacterial and Hemostatic Abilities of HA-EPL Coacervates
Bacterial infection will delay the wound healing process, so an ideal wound dressing should possess excellent antibacterial activity[36]. In this case, the antibacterial activity of HA-EPL coacervates against S. aureus (gram-positive bacterium) and E. coli (gram-negative bacterium) was evaluated via surface antibacterial activity tests. Following incubation for 1 h, more than 85% of S. aureus was killed by 4%, 6%, and 8% HA-EPL (Fig. 4a and 4b), thus demonstrating the excellent antibacterial ability of HA-EPL coacervates against S. aureus. Notably, only 6% and 8% HA-EPL exhibited outstanding bacteriostatic effects for E. coli, whereas 4% HA-EPL showed a poor bacteriostatic effect (Fig. 4a and 4c). In general, because of the differences in the cell wall and cell membrane structure between Gram-negative and Gram-positive bacteria, EPL was more sensitive to Gram-positive bacteria, meaning that HA-EPL coacervates had a better killing effect on S. aureus[37, 38]. Furthermore, the bacteriostatic effect was enhanced by increasing the relative content of EPL in HA-EPL coacervates. After examining previous experimental results, 8% HA-EPL was chosen for subsequent experiments owing to its better antibacterial ability and excellent mechanical properties.
The coagulation efficacy of samples was evaluated via a tube reversion test. As displayed in Figure S7, the precursor solution of 8% HA-EPL could not coagulate heparinized rat whole blood completely, while 8% HA-EPL itself could form a blood-hybrid coacervate. This was because positively charged EPL formed flocs with negatively charged blood cells. Furthermore, the in vivo hemostatic performance of 8% HA-EPL was evaluated by the rat liver bleeding model and the mouse tail-amputation model. For both bleeding models,8% HA-EPL exhibited excellent hemostatic performance. In the mouse tail-amputation model, the blood loss of the 8% HA-EPL group was significantly reduced compared with that of the control group (Fig. 4d). Correspondingly, the quantitative analysis results indicated that the blood loss in the 8% HA-EPL group (83 mg) was remarkably less than that in the control group (284 mg). Besides, 8% HA-EPL exhibited good hemostatic ability in the rat liver bleeding model. As shown in Fig. 4e and Movie S4, 8% HA-EPL immediately adhered to the wound surface and sealed the open blood vessels after liver resection. Only a little bleeding was observed during this process, significantly different from the control group. According to the quantitative analysis, the blood loss was 421 mg in the control group and only 102 mg after treatment with 8% HA-EPL (P < 0.001), illustrating the good hemostatic effect of the 8% HA-EPL.
3.4. Toxicity Evaluation
The safety of dressings is a prerequisite for application. First, we evaluated the cytotoxicity of HA-EPL coacervates via MTT assay. As depicted in Figure S8, with an increasing concentration of HA-EPL coacervates, the cell viability was similar, which was higher than 80%. This result showed that HA-EPL coacervates had low cytotoxicity and good biocompatibility. Besides, after treatment with 8% HA-EPL, major organs were collected for organ toxicity evaluation. As illustrated in Figure S9, there was no significant difference between normal and HA-EPL groups. No obvious tissue degeneration or necrosis was found after treatment with 8% HA-EPL. In conclusion, these results showed that HA-EPL coacervates possessed excellent safety, which could be used as an ideal dressing.
3.5. In vivo Full-thickness Wound Healing
The above results proved that 8% HA-EPL possessed desirable properties for an ideal wound dressing. Thus, we evaluated the efficiency of 8% HA-EPL using a mouse full-thickness skin defect model. Dorsal full-thickness skin wounds with a diameter of 10 mm were created and subsequently treated with control (untreated group), Tegaderm film (3M group), and 8% HA-EPL (HA-EPL group), respectively. Representative pictures of wounds in each group at predetermined times are summarized in Fig. 5a. Macroscopically, the therapeutic effect of the HA-EPL group was better than that of the untreated group and 3M group (Fig. 5a and 5b). Correspondingly, the wound areas at predetermined times were quantitatively measured (Fig. 5c). On the fifth day, the wound contraction in the HA-EPL group was most pronounced, with a relative healing area of 47.36%, which was higher than that in untreated (33.44%) and 3M (38.86%) groups. After healing for ten days, all the wounds exhibited significant contraction, and the wound contraction in the HA-EPL group was still higher than that in the untreated group and the 3M group (P < 0.05). The wounds of three groups were almost completely repaired after 15 days, but the wounds treated with 8% HA-EPL were still better than other groups. Besides, the results of H&E staining and Masson staining suggested that 8% HA-EPL effectively downregulated inflammation and recovered the skin structure closer to its pre-injury state (Figure S10 and S11). These results indicated desirable properties endowed 8% HA-EPL with the best healing efficiency.
Cytokines are highly correlated with wound healing, which can indirectly reflect the therapeutic effect of dressings and the healing quality of wounds[39]. Therefore, some cytokines were chosen as indicators of wound healing. Here, tumor necrosis factor-α (TNF-α) was selected to investigate the inflammation of new tissues. Compared with the untreated group, lower expression of TNF-α was observed in the 3M and HA-EPL groups (Fig. 5d), indicating that both Tegaderm Film and 8% HA-EPL could reduce the inflammatory response. In addition, the reconstruction of blood vessels can provide sufficient oxygen and nutrients for cells to accelerate the wound healing process[40]. Therefore, immunofluorescence staining of platelet endothelial cell adhesion molecule-1 (CD31) and vascular endothelial growth factor (VEGF) was carried out to evaluate angiogenesis and vasculogenesis. As expected, the HA-EPL group showed higher expression of VEGF and more pronounced angiogenesis (Fig. 5d and Figure S12). Subsequently, we performed immunofluorescence staining of collagen I (Col-I) and collagen III (Col-III). Better collagen deposition was found after treatment with the Tegaderm Film and 8% HA-EPL, which illustrated their good ability to promote healing (Figure S13and S14). In summary, in terms of relative healing area, inflammatory response, collagen deposition, and vascular reconstruction, 8% HA-EPL exhibited a better ability to promote healing than the other two groups.
3.6. In vivo Full-thickness Infected Wound Healing
According to the results of antibacterial tests in vitro and full-thickness wound healing in vivo, 8% HA-EPL showed excellent effects in bacteriostasis and the promotion of wound healing. Therefore, a full-thickness infected skin defect model was established to evaluate the potential application of 8% HA-EPL. As depicted in Fig. 6a and 6b, after healing for three days, wound contraction in the HA-EPL group was more obvious than that in the other groups (P < 0.01). Correspondingly, the number of S. aureus colonized in the wound decreased nearly tenfold compared with the other two groups (Fig. 6d and 6e; P < 0.001), thus demonstrating the remarkable antibacterial ability of 8% HA-EPL. Similarly, on the seventh and tenth days, the therapeutic effect of the HA-EPL group was also better than that of the untreated group and the 3M group (P < 0.05). Furthermore, the 3M group still showed pathogen contamination (P < 0.05), while the S. aureus was almost cleared in the HA-EPL group. Overall, the antibacterial ability of 8% HA-EPL resulted in a significant difference in wound healing rates compared with other groups.
Similarly, H&E and Masson staining were performed to evaluate the effect of 8% HA-EPL. As displayed in Fig. 6f, on the third day, enhanced inflammatory infiltration was observed in both the untreated and 3M groups. Comparatively, the inflammatory infiltration was significantly suppressed, and more fibroblasts were gathered around the impaired region. The colonization of bacteria in the wound prolongs the inflammatory period and delays wound healing. The excellent antibacterial activity from 8% HA-EPL was found to eliminate bacteria and downregulate inflammation, which might enter the proliferation period early. This result was also confirmed by Gram staining. On the third day, obvious bacterial colonization was found in the wound bed and the skin appendages (sweat glands, etc.) of normal tissue in both the untreated and 3M groups, while in the HA-EPL group, the bacterial colonization was significantly reduced and no infection of the appendages was observed (Figure S15). On the seventh day, inflammatory infiltration remained in the untreated and 3M groups. However, the inflammatory infiltration disappeared, and the epidermis was visible in the HA-EPL group (Fig. 6f). Additionally, residual scabs were still found in both the untreated and 3M groups, which indicated the delayed healing process of infected wounds. Meanwhile, compared with the untreated and 3M groups, there was obvious collagen deposition (Fig. 6g), and no obvious signs of infection were found in the HA-EPL group (Figure S15). After ten days of treatment, for the HA-EPL group, the wound had completely closed, and the epidermis was quite clear compared with the other two groups. Correspondingly, it was found that both the Tegaderm Film group and 8% HA-EPL group exhibited higher collagen deposition than that of the untreated group. In summary, 8% HA-EPL could shorten the healing time of S. aureus-infected wounds through efficient sterilization, downregulation of inflammation, and promoting collagen deposition.
The efficacy of 8% HA-EPL in preventing infection was firstly investigated via immunofluorescence staining of TNF-α in the wound bed (Fig. 7a and 7e). After ten days of treatment, TNF-α was still detected in the untreated and 3M groups, indicating a high level of inflammation at the wound site. In contrast, only a small amount of TNF-α was expressed in the HA-EPL group, suggesting that the inflammation and infection of the wound had been improved. This result could be attributed to the presence of EPL in 8% HA-EPL, which has been demonstrated to have broad-spectrum antibacterial properties. Furthermore, revascularization plays an important role in the wound healing process. As shown in Fig. 7b and 7f, a higher expression of VEGF was observed in the HA-EPL group. Similarly, double immunofluorescence staining of CD31 and α-smooth muscle actin (α-SMA) showed that the density of blood vessels in wound tissue significantly increased in the HA-EPL group (Fig. 7c and 7g), which illustrated the capability of 8% HA-EPL in recruiting host cells for angiogenesis[41]. In wound healing, fibroblasts secrete collagen to enhance the mechanical strength of the new skin. As depicted in Fig. 7d and 7h, fibroblasts in the HA-EPL group were abundantly recruited at the wound bed, and Masson staining additionally indicated that the collagen deposition was significantly higher than that in the other groups (Fig. 6g). In addition to preventing infection and reestablishing blood vessels, 8% HA-EPL also showed extraordinary advantages for epidermal regeneration and collagen deposition. After ten days of treatment, the wound in the HA-EPL group had formed an intact epidermis, almost surrounded by a layer of complete keratinocytes. However, in the untreated and 3M groups, only a few keratinocytes migrated to the wound bed (Figure S16). Furthermore, the expression of VEGF and inflammation-related genes were tested by q-PCR to demonstrate the advantage of 8% HA-EPL. As shown in Figure S17, the VEGF expression was significantly up-regulated in the HA-EPL group, and all inflammation factor expression including TNF-α and interleukin-1beta (IL-1β) was down-regulated after 8% HA-EPL treatment. These results suggested that 8% HA-EPL accelerated wound healing through the regulation of inflammation, collagen deposition, pro-vascularization and promoting the regeneration of the new epidermis.
{kind=link}