Treatment with thermosensitive liposomes and localized mild hyperthermia
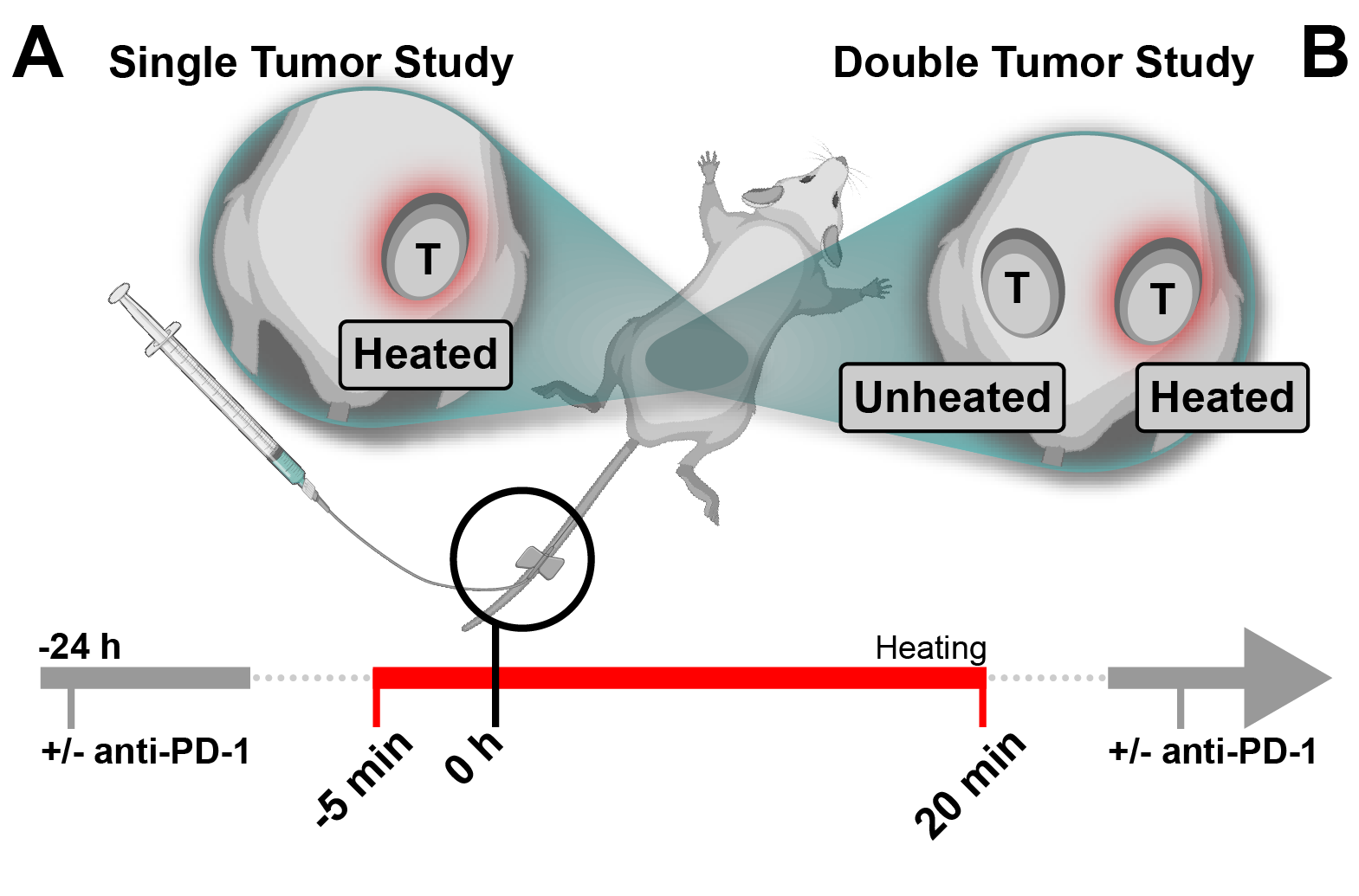
Systemic administration of thermosensitive liposomes in combination with localized mild hyperthermia has been proven to be highly effective in the treatment of local disease [41–43]. These improvements are largely attributed to increased accumulation and distribution of drug molecules at the tumor site [44–46]. However, this delivery approach requires heating of the target region as a trigger for drug release. Advances in heating techniques, thermometry, and treatment planning have significantly expanded the types, volumes, and locations of tumors that are amenable to mild hyperthermic heating [47–49]. Thus, expanding the clinical scenarios in which thermosensitive liposomes can be explored. However, any therapeutic approach focused on a localized target risks undertreating metastatic disease. Indeed, metastatic spread continues to be the primary cause of death from cancer [50, 51]. This raises the question of how to increase the systemic anti-tumor effects of this treatment approach. Previously, Viglianti et al. demonstrated that a formulation equivalent to ThermoDox was able to reduce tumor growth in secondary, unheated tumors in a bilateral immunodeficient mouse model [10]. The authors concluded that this effect “is most likely due to recirculation of intravascularly released drug” [10]. However, there are several factors that need to be considered prior to generalizing these findings. First, the drug’s pharmacokinetic properties will govern its circulation behaviour and thus impact systemic treatment effects. Second, it is important to note that this study employed water bath heating to achieve mild hyperthermic tumor temperatures. While this approach does lead to uniform heating of the animal’s hind limb, heating is not constrained to the tumor [52]. Consequently, drug release occurs throughout the entire heated vasculature. Differences in heated tissue volume have been shown to affect the kinetics as well as total amount of intravascularly released drug, thus leading to varied amounts of free drug present in the systemic circulation [52]. The laser-based heating setup employed in this study provides more precise localized heating compared to water bath heating [36]. Nonetheless, combining thermosensitive liposomal vinorelbine with localized mild hyperthermia treatment via this heating setup resulted in reduced growth of the contralateral (i.e., unheated) tumor. This reduction in tumor growth could be attributed to systemically available thermosensitive liposomal vinorelbine and free vinorelbine. However, since these studies were performed in an immunocompetent animal model, it could also be due to immune mediated anti-tumor effects stimulated by mild hyperthermia and/or vinorelbine chemotherapy. While it is interesting to observe this anti-tumor effect at the contralateral site, it is important to note that this is a bilateral tumor model used to assess systemic anti-tumor capabilities. In general, metastatic tumor cell spread follows a highly complex process that is not reflected by bilateral tumor implantation [53]. Nonetheless, following primarily localized drug release of vinorelbine at the heated tumor we do observe a systemic anti-tumor effect. Thus, this study confirms the findings reported by Viglianti et al., albeit in a different animal model, and for a different thermosensitive liposome formulation.
Immunocompetent animal models of rhabdomyosarcoma
We previously evaluated the combination of thermosensitive liposomal vinorelbine and mild hyperthermia in an immunocompromised murine model of RMS [39]. However, immunocompetent cancer models are necessary to evaluate the full potential of heat-triggered drug delivery approaches. While heating is used as the external trigger for drug release, it also elicits a series of effects that stimulate and enhance anti-tumor immune responses [26]. Most murine RMS models are based on human-derived xenografts and only a few syngeneic RMS animal models have been reported [54]. The M3–9-M RMS model employed was previously developed and characterized by Meadors et al. [35]. The authors demonstrated its immunogenicity and responsiveness to T-cell based immunotherapy [35]. Additionally, Highfill et al. demonstrated the role of PD-1 signaling in the immune escape of the M3–9-M tumors. Interestingly, in this study, PD-1 blockade therapy showed limited tumor growth inhibition effects when initiated later in the tumor development process [55]. Generally, orthotopic tumor models better recapitulate clinical disease, however, in the present study, tumors were grown subcutaneously due to limitations associated with the laser-based heating set-up [36, 56–58].
Previous studies combining thermosensitive liposomes and immune checkpoint inhibition
Kheirolomoom et al. have previously investigated similar strategies to increase the systemic treatment capabilities of thermosensitive liposomes. For example, the combination of a thermosensitive liposome formulation of doxorubicin with ultrasound mediated hyperthermia and intratumoral administration of CpG has previously been studied [59]. Here, CpG was employed as a local immune adjuvant to stimulate a more potent innate immune response. However, this therapy proved to be inefficient in treating distant (i.e., unheated) tumors. In a subsequent study, the authors showed that the addition of PD-1 blockade priming therapy to this treatment approach led to a potent anti-tumor T-cell response and successfully treated local as well as distant tumors [60]. The immunotherapy combination (i.e., i.t. CpG plus i.p. anti-PD-1) alone provided a potent systemic anti-tumor effect, without the addition of heat-triggered chemotherapy. Thus, based on this alone study, it is difficult to discern the contribution of thermosensitive liposomal doxorubicin to immunotherapy treatment. In our study, we also observed improvements in survival of animals receiving immunotherapy. Furthermore, we also see a significant survival benefit in animals treated with immunotherapy (i.e., anti-PD-1) in combination with thermosensitive liposomal vinorelbine and localized mild hyperthermia, compared to animals treated with immunotherapy alone. Albeit, in a different disease model and using a different treatment approach compared to the aforementioned study by Kheirolomoom et al. Ultimately, a comparison of the present study and the study conducted by Kheirolomoom et al highlights that the integration of immunotherapy into multimodal treatment regimens and evaluation of their efficacy in murine models of cancer is non-trivial.
Mild hyperthermia and abscopal effects
As mentioned previously, the exact mechanism underlying the abscopal effect associated with localized therapies remains unclear [20]. However, it is generally recognized that a systemic cytotoxic T-cell mediated anti-tumor response plays a key role. Interestingly, mild hyperthermia has been shown to directly and indirectly influence components of the innate as well as adaptive immune response [61]. However, it is important to note that in most of these studies heat is applied for extended periods of time (≥ 1 h) and/or whole-body hyperthermia is employed instead of localized heating. In fact, very few in vivo studies have evaluated the potential abscopal effects that may be induced by treatment with localized mild hyperthermia alone. Mild hyperthermia is most commonly applied in combination with chemotherapy or radiotherapy treatment, thereby making it difficult to determine any effect of mild hyperthermia alone [62, 63]. It was only recently that mild hyperthermia was combined with ICI to enhance abscopal effects [28, 64]. Oei et al. evaluated hyperthermia alone and in combination with ICI in a highly metastatic mouse model of breast cancer (i.e., luciferase transfected 4T1 cells). The authors observed an increase in lung metastases following treatment with a combination of localized mild hyperthermia and ICI (i.e., anti-PD-1 and anti-CTLA-4). In contrast, Ibuki et al. employed the non-transfected 4T1 parent cell line in a bilateral subcutaneous tumor model. Here the combination of mild hyperthermia and ICI (i.e., anti-CTLA-4) led to strong tumor growth inhibition of both heated and unheated tumors [64]. The combination treatment also reduced metastatic spread to lungs (compared to ICI alone), resulting in an increase in overall survival. The contradictory results reported by Oei et al. and Ibuki et al. further highlight the need for more research into the combined effect of immunotherapy and mild hyperthermia [28, 64]. While there are many differences in the study design and treatment strategies that might explain these results, there are four key differences that highlight the complexity of evaluating such a multimodal treatment approach. First, the immunogenic potential of the luciferase transfected cell line needs to be considered when evaluating an anti-tumor immune response [65]. Second, the anti-tumor immune response is heavily influenced and directed by the tumor microenvironment (i.e., orthotopic versus ectopic) [66]. Third, the immune effects mediated by mild hyperthermia treatment depend on the temperature and duration of heating as well as the specific heating technique [67, 68]. And lastly, the timing of treatment relative to disease burden is critical when evaluating the efficacy of treatment induced anti-tumor immune effects. For example, the overall tumor burden has been shown to have an immunosuppressive effect [69]. In the present study, when PD-1 blockade monotherapy was initiated early (i.e., at a significantly smaller tumor volume) this led to complete tumor remission (albeit n = 2 mice), while delayed treatment resulted in limited tumor growth inhibition (Figure S1). This is in agreement with the previous work done by Highfill et al [55]. These studies demonstrate the complexity of this multimodal approach and highlight the need for detailed studies to better understand the parameters that influence treatment outcomes.
Contributions of chemotherapy to systemic anti-tumor immune response
There is a growing body of evidence that suggests chemotherapy can exert a physiological response beyond a direct cytostatic or cytotoxic effect. In fact, some have proposed that the reason behind the success of certain chemotherapies lies in their ability to induce an anti-tumor immune response [70, 71]. This is usually attributed to a specific form of regulated cell death, known as immunogenic cell death [72]. Indeed, several commonly used chemotherapeutic drugs have recently been identified as immunogenic cell death inducers. Among these are anthracyclines (e.g., doxorubicin) as well as microtubule inhibitors (e.g., taxanes and vinca alkaloids), including vinorelbine [73–75]. The classification of chemotherapeutic drugs as immunogenic cell death inducers is an active area of research. However, there is evidence to suggest that both localized mild hyperthermia as well as vinorelbine chemotherapy can create immunogenic tumors [76–82]. This would certainly be advantageous, and potentially synergistic, when administered in combination with ICI therapy. In the present study, such synergy is observed for the triple combination of thermosensitive liposomal vinorelbine, mild hyperthermia, and anti-PD-1. Specifically, this is demonstrated by enhanced efficacy at the distant tumor sites. Furthermore, this idea of exploiting the potentially immunostimulatory effects of vinorelbine is currently being investigated in clinical trials as a combination with immunotherapy (NCT03801304, NCT03518606, NCT04848454).
To conclude, thermosensitive liposomal vinorelbine plus localized mild hyperthermia in a bilateral tumor model of RMS was shown to have a significant anti-tumor effect at the heated primary site, resulting in tumor remission. Moreover, an effect at distant tumor sites was also observed for this treatment approach, albeit limited to reduced tumor growth rates. Interestingly, combining immune checkpoint inhibition therapy with thermosensitive liposomal vinorelbine and mild hyperthermia significantly improved treatment of distant tumor sites. Moreover, the addition of immune checkpoint inhibition therapy to localized mild hyperthermia alone produced a measurable abscopal effect. The underlying mechanism of this synergistic treatment effect will require further investigation. Yet, to the authors knowledge, this is the first study demonstrating that immune checkpoint inhibition therapy alone can enhance the systemic treatment capabilities of thermosensitive liposomes in combination with localized mild hyperthermia.
{kind=link}
{kind=link}