Potential complications can be prevented with early diagnosis and treatment even in asymptomatic cases [10]. Hydatid cyst is a disease requiring treatment irrespective of the diameter or stage. The incidental diagnosis of the majority of the patients operated on in our clinic with no symptoms and prompt treatment reduces the risk of the cyst opening to the bile ducts and rupture.
The basic aim in the treatment of hydatid cyst is to relieve symptoms such as infection, obstructive jaundice, and anaphylactic shock that may result from cyst rupture and to prevent complications [11]. This is done by inactivating and removing all viable scolices and germinal membranes and by managing the residual cavity with minimal morbidity and mortality [5, 6, 12]. The best means of achieving this and minimizing recurrence and complications is through surgery. In addition, total elimination of the parasite in the treatment of hydatid cyst also relies on the absence of intraoperative shedding and the preservation of healthy tissues [13]. In contrast to surgery, intraoperative shedding develops beyond our control in PAIR, and chemotherapy is required in order to cope with potential complications. In our clinic, before surgical treatment, contact between the contents of the cyst and the abdominal wall and internal organs is prevented by wrapping the cyst with compresses moistened with scolicidal agent.
The methods employed in the treatment of HCL include chemotherapy, percutaneous procedures, and surgery [10].
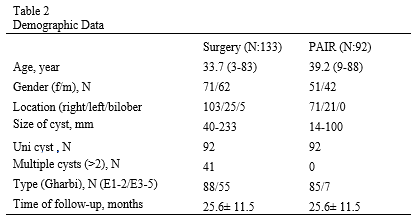
Indication of surgery depends on the nature of the cyst and the patient’s general condition [12, 13]. Surgery remains the standard treatment due to the largely inadequate effects of medical therapies and the complications of percutaneous techniques [7, 9, 13]. Surgical treatment is also our first choice, since we regard it as more effective, since we are in an endemic region, and due to the morphology of the cyst. The surgical approach is usually preferred in large cysts with multiple offspring cysts, complicated cysts (such as rupture, biliary fistulas, compression of contiguous vital structures, bacterial infection, and bleeding), and superficial cysts [7, 14]. Surgical procedures were performed due to cyst diameters exceeding 100 mm in 57 of our patients who underwent open surgery, multilocular cysts in 45, multiple cysts in 36, and biliary tract involvement in five, superficial cyst in one, and contiguity to the vena cava in one.
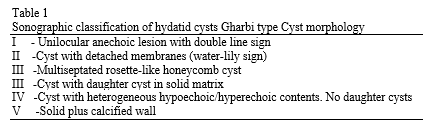
PAIR has been found to be particularly effective and safe in the treatment of Gharbi type 1 and 2 cysts [6]. However, it cannot be performed on all cysts at this stage. It applicability is affected by the location and the morphology of the cyst. The PAIR procedure may be regarded as suitable for cysts > 50 mm and Gharbi type 1 and 2 cysts.[7] PAIR is only a good option for univesicular cysts with a significant fluid component with an intact endocyst and absence of biliary communication [15]. Cholangiography was performed pre-procedurally in all our cases, and PAIR was not applied if biliary fistula was suspected. In our cases, it was mostly applied to Gharbi types 1 and 2 and a smaller number of type 3 cysts, between 20–100 mm in diameter, which were univesicular, not superficial, and with no wall calcification or biliary involvement.
It can be performed on patients who refuse surgery or with a high anesthesia risk. However, we recommend retreatment with surgery in cases of postsurgical recurrence. Additionally, we do not recommend PAIR unless success has been achieved with chemotherapy, because chemotherapy is used to prevent hydatidosis and recurrence caused by leakage during PAIR. Complications may increase after PAIR if chemotherapy has been ineffective.
Recurrence was determined in four of the 17 patients with cyst diameters > 50 mm. Small diameter is not an obstacle in experienced clinics. The important factors are the stage of the cyst, location site biliary involvement, and that the diameter should not exceed 100 mm. Although PAIR was not performed in large, multi-cystic, multi-local patients associated with biliary involvement before the procedure, our recurrence rate was significantly higher than in open surgery. This high rate may have been due to deficient preoperative evaluation, inadequate evacuation of the cyst content, an adequate scolicidal concentration not being achieved, a short duration of exposure to injected hypertonic fluid, or lack of contact with part of the offspring cysts. The experience of the radiologist performing the procedure and the imaging device employed may also affect the quality.
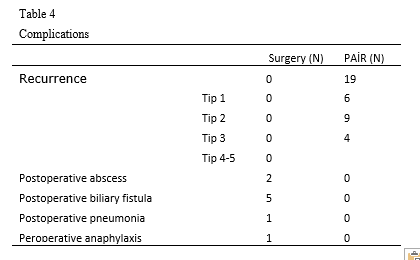
Occurrence developed in 17.6% of the 85 patients (15) with Gharbi type 1–2 cysts who underwent the PAIR procedure in this study. Our failure rate among patients at this stage was low. The most important disadvantage of the PAIR technique us that the hypertonic saline infusion and injected alcohol cannot be aspirated during to separation of the membranes [11]. Aspiration can increase recurrence rates in case of multilocular and numerous offspring cysts. Success rates are low (39%) in Gharbi type 3 cysts due to the cyst content [6, 11]. Seven of our patents were Gharbi type 3, and recurrence developed at the high rate of 57.1% (4) in these. We do not therefore recommend PAIR in Gharbi type 3 cysts. In contrast to the previous literature, the PAIR recurrence rate in the present study was 20.6% (N:19), while no recurrence was observed in open surgery. Surgery may represent a definite solution in the treatment of recurrences.
In our clinic, chemotherapy is not employed, except in case of spread of the cyst content into the abdomen during PAIR, rupture, and surgery. Albendazole together percutaneous drainage is thought to be a safe and effective method for treating hydatid cyst [16]. Our recurrence rate may have been high due to an insufficient duration of chemotherapy following PAIR. Albendazole taken at 800 mg twice daily day for at least six to 12 months after surgery may play an interesting role in preventing recurrence [17].
However, we recommend chemotherapy in the event of the cyst fluid spreading to the abdomen in open surgery. Chemotherapy was applied for eight weeks postoperatively to three of our patients presenting due to perforation. We attribute the absence of recurrence during the follow-up of patients operated due to perforation to careful exploration, removal of all cyst tissues from the body, and the effect of drainage and chemotherapy. The noteworthy point here is the great difference in terms of recurrence compared with PAIR even though a large part of the abdomen was contaminated by cyst content after perforation. The duration of chemotherapy is the same in perforation and PAIR. Our success in perfusion is due to our observance of the rule of complete elimination of the cyst, the principal objective in the treatment of cyst. In other words, removing all the structures inside the cyst, rather than inactivating it, is an effective form of treatment. Surgery therefore remains the first choice treatment in our endemic region.
Surgical treatment was performed in case of superficial cysts, rupture or cysts with a major extrahepatic component, cysts close to vessels, and those with biliary involvement or suspicion thereof, irrespective of stage or diameter.
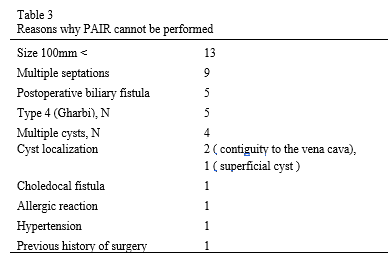
Since HCL is endemic in our region, and since presentations usually involve large and complicated cysts, the PAIR procedure is not particularly appropriate. The low number of PAIR procedures derives largely from patient preferences for surgery because of the pandemic and the nature of the cyst. One hundred thirty-five of the 225 patients were referred to the radiology department for the PAIR procedure. However, 43 of these were reported as unsuitable and were referred to the surgery department, and surgical treatment was applied with no complications. Reasons for unsuitability are shown in Table 3. Our high recurrence rate after PAIR encourages us to avoid conservative treatment.
However, we encountered no mortality or morbidity in the 133 operated patients in this study. There was also no recurrence, the most important post-operative complication, with only biliary fistula being observed. Some large-scale studies have reported lower morbidity with resectional surgery than with conservative procedures [9]. Our findings are consistent with those studies.
The most frequent complications of HCLs are infection and cyst rupture into the biliary tree [18]. Rupture into the choledocum was present before surgery in one of our patients. That patient was operated using ERCP, and no complication developed. Rupture into the small bile ducts is asymptomatic and most cases can be detected during surgery. Perioperative bile leakage was present in 21 of our 133 operated patients, and this was sutured using number 3/0 polypropylene. Postoperative biliary fistula developed in two of these patients.
Surgical procedures were performed on five patients with biliary involvement at cholangiography carried out prior to PAIR. Since no fistula was detected perioperatively in any of these patients, no additional fistula-oriented intervention was performed. Bile fluid emerged from the drain in two of the five patients in the postoperative period. Management of postoperative bile leakage often requires sphincterotomy and the use of invasive procedures such as stenting or percutaneous drainage, which may be associated with morbidity and even mortality [9]. ERCP was applied to three patients producing 200 cc of postoperative bile from the drain, to two who underwent fistula interventions during surgery, and to one suspected case during PAIR but in which no perioperative fistula was observed, while bile flow ceased spontaneously in two patients.
Biliary fistulas that do not close spontaneously or with ERCP can be easily detected without any procedure during open surgery due to their high flow rate. Both short- and long-term postoperative morbidity, bile leakage, and recurrence risks are significantly low in surgical treatment [19]. We do not therefore recommend any additional procedure for investigating biliary fistulas that are not seen perioperatively. Our open surgery biliary fistula rate is 0.015%. Abscess developed in two patients after surgery. It were drained percutaneously.
When PAIR is performed at Type 4 and Type 5, we do not recommend at this stage, due to the high rate of bile leakage and since severe post-operative complications will increase. Our aim must be to determine the most appropriate mode of treatment while causing minimal damage to healthy tissue. The foundation stone in the treatment of HCL is surgery [13]. We recommend Cystectomy as a surgical technique in endemic regions, since this is safe with minimal complications. It should definitely not be applied to superficial cysts, as the spread of the cyst material from the needle insertion site causes anaphylaxis and widespread cysts in the abdomen.
The most feared complication of percutaneous treatment of hydatid disease is fatal anaphylactic shock [20]. No fatal anaphylactic shock was observed in the present study, although reversible anaphylactic shock was encountered during open surgery in one case. Care must be taken during PAIR, and it should always be remembered that such complications may develop with wither PAIR or open surgery in the treatment of hydatid cysts.
Less frequent complications include intraperitoneal rupture [18]. Rupture may result in pressure necrosis due to trauma or relentless expansion of the hydatid cyst, leading to rupture into the peritoneal cavity, pleural cavity, or bile duct [9, 18]. Rupture into the bile ducts was determined in one patient in our clinic, and intraperitoneal rupture in three. We think that spontaneous cyst development in three patients was due to increased pressure within the cyst. Intraperitoneal rupture developed due to a fall in one patient. Hydatid cyst rupture should therefore always be considered in endemic regions, especially in patients presenting with abdominal pain as a result of trauma with a history of HCL. No symptoms other than abdominal pain were present in three patients presenting to our emergency surgery unit due to rupture. Such complications may not be caused if abdominal exploration is well performed during surgery in cases operated due to rupture and when albendazole is administered at appropriate doses and time frames.
Length of hospital stay depends on the treatment selection. Lengths of stay of 1–4 days have been reported with the percutaneous approach and of 6–15 days for surgery [10]. Our patients undergoing PAIR were hospitalized for three days each. The mean length of stay with open surgery was 7.3 days. However, PAIR also entails such disadvantages as a high recurrence rate and rehospitalization for treatment.
{kind=link}
{kind=link}
{kind=link}
{kind=link}