HBV, HCV and chronic cholangitis contribute to the majority of the 70,000 ICC cases emerging in China1, revealing the heterogeneity of Chinese cases with those of Westerners and South East Asians. Multiple studies have investigated the molecular profiles of cholangiocarcinoma in Western countries, but genetic information for Chinese patients with ICC is lacking. In this study, 417 cancer-associated genes from 122 ICC patient samples were subjected to NGS, and a genetic profile was obtained. TP53, KRAS and ARID1A were identified as commonly occurring genetic alterations, similar to the results of the present study (table 2).
Genomic alterations, mostly rearrangements, in FGFR2 are commonly reported in cholangiocarcinoma patients in Western countries12,13, and these alterations result in constitutive activation of the FGFR2 receptor. In this study, a much lower FGFR2 alteration rate (2%) was detected in the Chinese population compared with that in other populations. Patients with FGFR fusion could benefit from BGJ398 and derazantinib treatment, and prospective clinical trials are evaluating the efficacy of multiple anti-FGFR treatments on cholangiocarcinoma (NCT04093362/NCT02924376/NCT03773302/NCT04238715/NCT02150967/NCT03230318/NCT03656536/NCT04088188).
ERBB2 amplifications are relatively rare in ICC compared with other types of biliary tract cancer (BTC)14. Due to low mortality and the number of patients with specific ERBB2 amplifications, a previous clinical trial (NCT00478140) was halted. The frequency of ERBB2 amplification in this study was 8%, which is higher than that previously reported by other studies14. Notably, the disease control rate among eight patients who received anti-ERBB2 treatment with trastuzumab reached 7/8, and one patient achieved a clinically resectable status. The therapeutic efficacy of anti-ERBB2 agents on ERBB2-amplified ICCs has not been previously reported, but phase II trials in China and South Korea are set to evaluate the combination of gemcitabine-based chemotherapy with tastuzumab in cases of ERBB2-amplified extrahepatic cholangiocarcinoma and gallbladder cancer (NCT02836847) and BTC (NCT03613168). Basket and multicenter trials may evaluate this treatment more adequately.
Cholangiocarcinoma patients with BRCA1/2 mutations treated with PARP inhibitors exhibited a favorable response15. The predictive features of germline and somatic mutations remain to be elucidated, and the germline versus somatic mutation ratio in this study was 2:12. In this study, only four patients accepted olaparib treatment, mostly due to economic factors. A recent study demonstrated that the accumulation of 2-hydroxyglutarate in association with isocitrate dehydrogenase (IDH) mutations can suppress homologous recombination and thereby induce sensitivity to PARP inhibitors16. These findings provided the foundation for a trial exploring the antitumoral activity of olaparib in solid tumors that harbor IDH1/2 mutations (NCT03212274). IDH1/2 alterations are frequently reported in ICC, and 13 (11%) patients with IDH1 mutations and 6 (5%) patients with IDH2 mutations were included in this study. Ongoing studies are evaluating the IDH1 inhibitors ivosidenib (NCT02989857) and BAY 1436032 (NCT02746081) in BTC. However, because these IDH inhibiters are not available at our center, our patients did not have the opportunity to receive anti-IDH treatments.
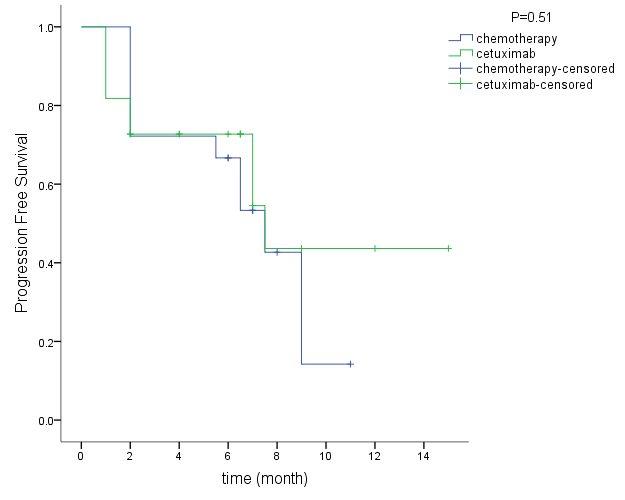
In this study, compared with those in the chemotherapy alone group, the partial response and stable disease rates were higher and the PFS time was longer in cetuximab treated patients; however, the differences were not statistically significant. These results were obtained from patients with wild-type KRAS/NRAS/BRAF genes. Both NRAS and BRAF were altered in 3 (2%) patients, and this rate was much lower than that of KRAS alterations (31 patients, 25%). Previous clinical trials indicated that EGFR inhibitors, including cetuximab and erlotinib, do not improve the therapeutic efficacy of gemcitabine-based chemotherapy, although they are well tolerated17,18. One study indicated that the KRAS status was not associated with PFS in cholangiocarcinoma patients treated with both gemcitabine and cetuximab, but the patient sample number was limited19. A phase II study reported that panitumumab combined with gemcitabine and oxaliplatin (GEMOX) had a good therapeutic efficacy in KRAS wild-type patients, who exhibited a good survival time20. Our results support further investigations of the administration of EGFR inhibiters to KRAS wild-type patients.
The disease control rate (85%) and response rate (60%) achieved with bevacizumab treatment combined with chemotherapy in this study as well as the prolonged PFS time (15.4 months) are encouraging. The survival data of patients treated with this combination were significantly better than those of patients in the chemotherapy group. Moreover, two of the patients exhibited complete responses, and 10 patients underwent hepatectomy after systemic therapy. However, the evidence for adding bevacizumab to gemcitabine-based first-line chemotherapy is still insufficient and comparatively weak. Zhu et al assessed the efficacy of bevacizumab in combination with GEMOX in 35 patients with advanced BTCs, and the reported PFS rate at 6 months was 63%, which was satisfactory but below the targeted rate of 70%21. Iyer et al explored the efficacy of bevacizumab combined with gemcitabine-capecitabine in 50 patients with advanced BTCs, reporting a PFS time of 8.1 months, an OS time of 10.2 months and a clinical benefit rate of 72%22. However, concluding that the addition of bevacizumab improved outcomes was not possible based on the results. A controlled clinical trial reported longer PFS times in the bevacizumab combination group (6.48 months) than in the GEMOX group (3.72 months)23. There are cases of ICCs being successfully treated with bevacizumab combined with oxaliplatin-based chemotherapies as a consequence of misdiagnosed colorectal carcinoma liver metastasis24,25. Evidence supporting neoadjuvant or conversional treatment in ICC is lacking, but our results showed that late staged patients accepted combination of chemotherapy and bevacizumab treatment and consecutive operation had a longer PFS time than those underwent radical surgery. Patients may benefit from pre-operation systemic treatment. Thus, bevacizumab is an underutilized target agent for ICCs, and its efficacy and safety should be further evaluated.
The reported frequency of MSI-H in cholangiocarcinoma patients ranges widely from 1% to 10%26,27, and a prospective study reported an MSI-H rate of 0.5% in unselected cholangiocarcinoma patients12. In this study, the MSI-H rate was 2% in ICC patients; both patients accepted immunotherapy with pembrolizumab, and the therapeutic efficacy was satisfactory. The FDA approved pembrolizumab for the treatment of MSI-H/mismatch repair deficient (dMMR) tumors, which showed a predictive response to immunotherapy with PD–1 checkpoint inhibitors28. The KEYNOTE16 phase II study reported a 100% disease control rate for 4 MSI-H cholangiocarcinoma patients who received pembrolizumab29, and ongoing clinical trials are accessing immunotherapy in combination with chemotherapy (NCT03111732) or radiotherapy (NCT03898895) for the treatment of cholangiocarcinoma. Additionally, a trial has been designed that combines a PD–1 antibody, a tyrosine kinase inhibitor (TKI, lenvatinib) and GEMOX for the treatment of ICCs (NCT0395197). All studies accessing the therapeutic efficacies of TKIs (including the multitarget TKIs cabozantinib30, vandetanib31, sorafenib32; the panErbB family receptor TKI afatinib33; the VEGF family receptor TKI cediranib34; and the combination of pazopanib and trametinib35) failed to show survival improvements. The use of checkpoint inhibitor and TKIs in combination may bring hope to patients with ICC.
This study was retrospective, which limits its evidence grade. However, we herein integrated the genetic profiles of ICC patients in the Chinese population. To our knowledge, this is the largest study on the use of NGS results as a reference for selecting target/immune therapies.
{kind=link}