In this study, we evaluated the effect of time to primary repair on visual acuity outcomes of OGI injuries repaired within 24 hours who presented to a single academic institution. Our results indicated that there was no significant correlation between time to OR and final visual acuity within the 24-hour window. This study also supports previous data that found significant association of other factors with visual acuity outcomes.
The finding that time to primary operative repair within the 24-hour window does not have a discernible impact on visual outcomes is a clinically important finding. While situations will arise that call for an ophthalmologist to use their judgment and take an OGI for primary repair immediately, there are many reasons why an ophthalmologist may wish to instead delay an OGI repair with a goal of repair within the 24-hour period, including patient hemodynamic stabilization after trauma, or insufficient OR and anesthesia staffing overnight or on weekends. In addition, there are factors outside of a surgeon’s control that may delay primary OGI repair, such as delays in transfer of the patient from an outside hospital. Given the results of our findings, we can conclude that delay in primary repair within the 24-hour post-injury window does not appear to have a statistically significant impact on final visual acuity on average and optimizing the patient and surgical environment is warranted to improve operative success and patient outcomes.
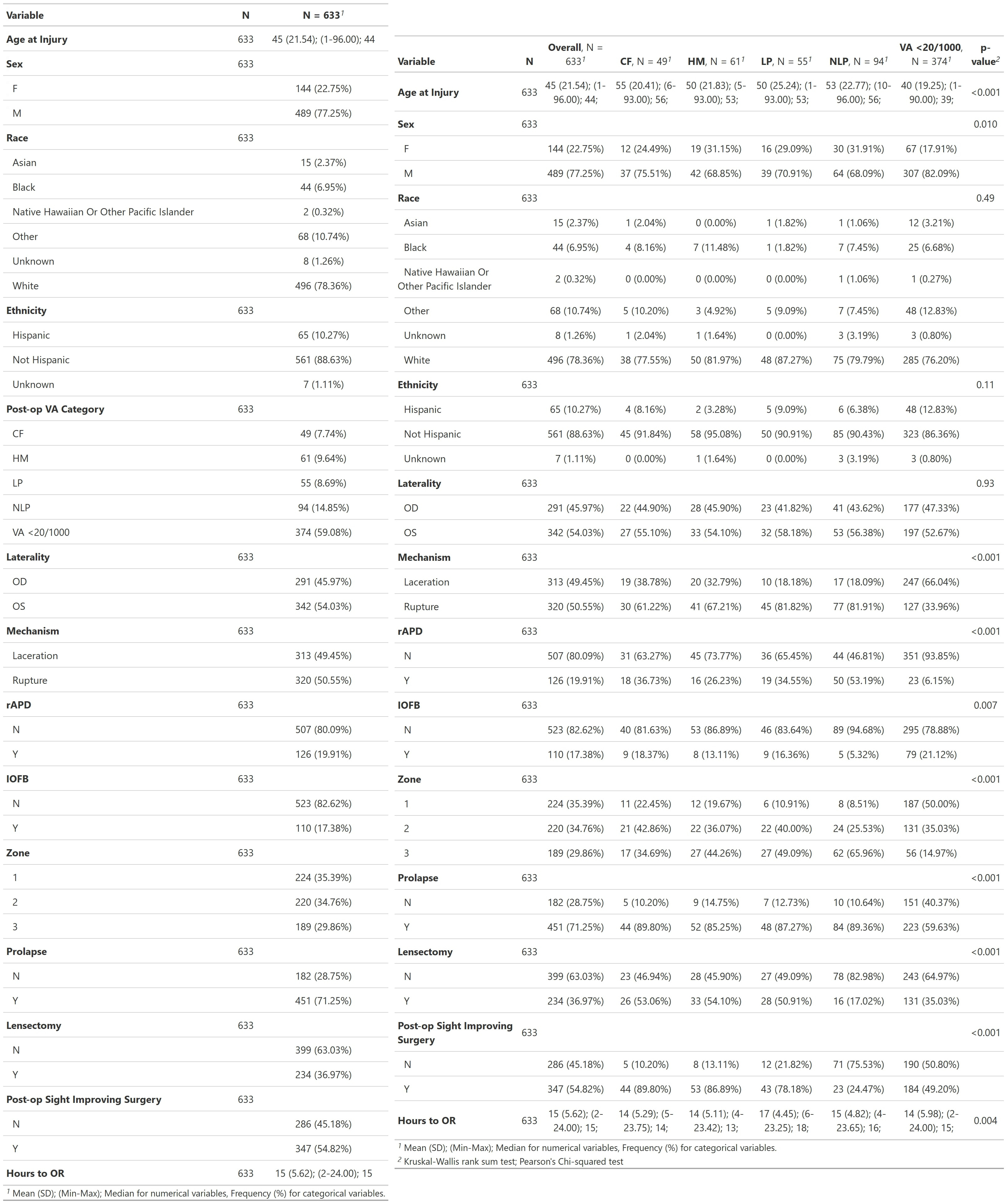
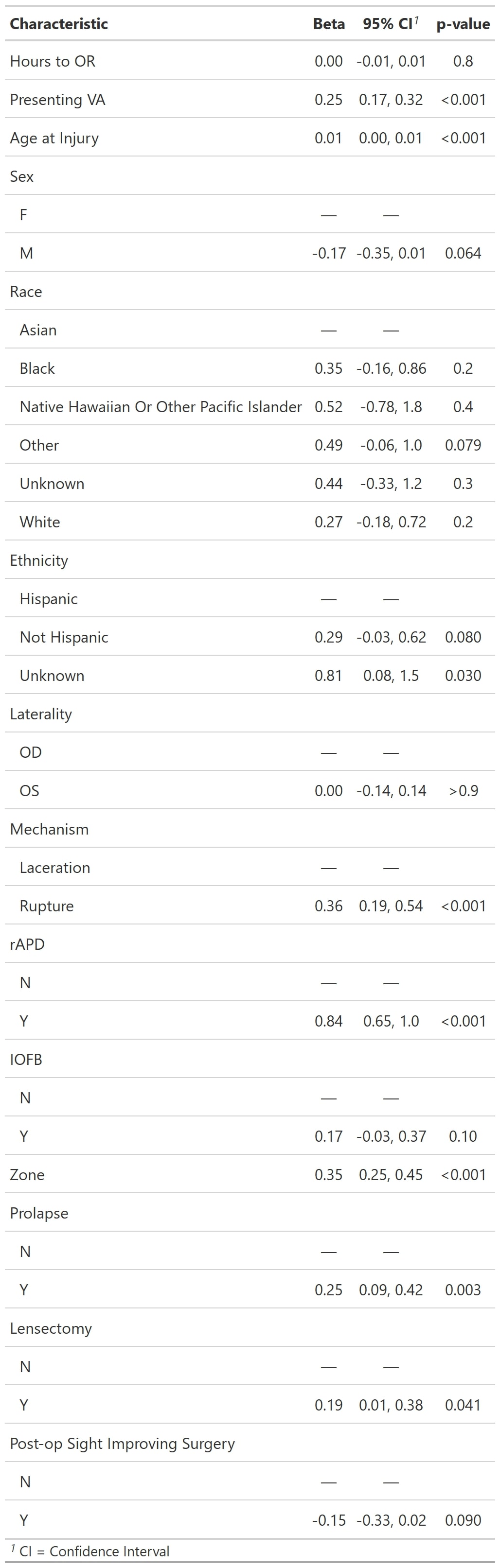
It is worth noting that variables other than time to operative repair influenced final visual outcome of patients with OGIs repaired within 24 hours, namely: presence of rAPD, rupture as mechanism of injury, presenting VA, higher zone of injury, uveal prolapse, and age at time of injury. This is consistent with prior literature where many of these factors were found to influence final visual acuity and were included in the Ocular Trauma Score, which can be used to prognosticate final visual acuity.2,3,4,5,6,7,8,20 Notably, in our study, presence of rAPD was the strongest predictor of poor final visual acuity, followed by rupture as a mechanism of injury. Mechanism of injury was also highly correlated with visual outcomes, with only 8.6% of laceration injuries resulting in LP or worse vision, versus 38% of rupture injuries resulting in LP or worse vision. Notably, all of these factors are intrinsic to the patient or the nature of the injury, and none are able to be controlled by the ophthalmologist. In addition, while presence of IOFB has been shown previously to be a risk factor for endophthalmitis,10 presence of IOFB did not correlate significantly with worse final visual acuity in our study.
While time to primary repair of OGI did not correlate with visual outcomes, we did identify interesting trends in the practice patterns of OGI repair at our institution. We found that eyes with Zone 3 injuries were treated 1.67 hours later on average than those with Zone 1 or 2 injuries (p = 0.005). Meanwhile, eyes with rupture as a mechanism were treated 1.5 hours later on average than those with laceration injuries (p = 0.002). This may be due to either patient factors such as more severe comorbid trauma occurring with blunt ruptures, or physicians’ understanding of the poorer prognosis associated with blunt rupture and Zone 3 injuries.
Limitations of this study include its retrospective nature and single-center design. However, inclusion of consecutive patients over a ten-year period who were treated by multiple surgeons increases the generalizability. Selection bias may also exist, as MEE is a major referral center that may see and treat more advanced ocular trauma. While we only evaluated patients treated within the 24-hour window, we see this as a critical strength of our study design, as the general practice pattern of ophthalmologists is to treat OGIs within the 24-hour window for endophthalmitis risk reduction.14 Therefore, OGIs repaired outside of the 24-hour window were purposely excluded. The predominance of white, non-Hispanic patients is representative of the population served at Massachusetts Eye and Ear but is not representative of the U.S. and global population of those who sustain OGIs. Lastly, data analyzed included only initial and final vision, which did not take into account changes in vision in the interim, as some final follow-up visits were many months or years after the primary OGI repair.
In conclusion, while OGIs have the potential to inflict severe ocular and visual morbidity, our findings suggest that time to primary operative repair of OGIs does not influence final VA if repaired within the 24-hour window. Other variables which impact final VA include rAPD, rupture as a mechanism, presenting VA, higher zone of injury, uveal prolapse, and age at time of injury, as is consistent with prior literature. Ultimately, optimization of patient and surgical factors, as well as individualized, longitudinal treatment plans for patients with OGI, likely has a more meaningful impact on patient visual acuity outcomes than time to primary repair.
{kind=link}
{kind=link}