Magnetic resonance imaging has been shown to be superior to ultrasonography and computed tomography in determining the morphological features of tumoral tissues such as size, spread and relationship with vascular structures. 3 Also, muscle, tendon, cartilage, disc, meniscus, synovium, nerve, vascular, fat, fluid, cortical bone and bone marrow structures can be distinguished by MRI. Although unenhanced MRI is an important diagnostic tool in the evaluation of soft tissue masses, spread of lesions, staging of tumors, biopsy planning, preoperative chemotherapy response and recurrence-residual tissue can be detected with contrast enhanced MRI. 4
In our study, when we look at the frequency of head and neck masses according to their malignant and benign characteristics; It was determined that 33.3% of them were benign and 66.7% of them were malignant masses. When the relationship of the masses with gender is evaluated; similar to the literature, malignant masses in the head and neck region were found to be more common in men (58.8%), and benign masses were more common in women (67.6%) 5,6
Using MRI features (homogeneity and signal intensity in T1 and T2-weighted images, contrast enhancement pattern, margin feature, invasion status, presence of septation and lobulation, presence of cystic / necrotic area and bone involvement) of soft tissue masses to differentiate benign and malignant that very different results have been obtained by researchers. 7–13 The intensity and homogeneity of the MR signals in different pulse sequences are widely used in the detection of malignancy of the masses. 14 Weatherall et al. stated that high signal intensity in T2-weighted images is a sensitive parameter in the detection of malignant masses but has unacceptably low specificity. 15 Hermann et al. obtained as hypointense appearance in 17% and hyperintense appearance in 58% of benign tumors on T1-weighted images also hyperintense appearance in 85% of benign tumors on T2-weighted images. They found that malignant tumors exhibited hyperintense signal in 40% of T1-weighted images and in all T2-weighted images. 16
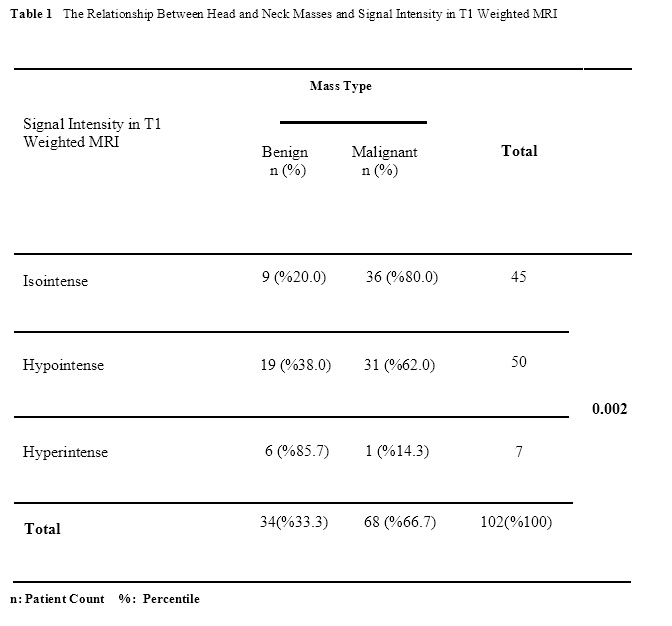
In our study, similar to the literature, we obtained hypointense signal intensity in 55.8% of benign lesions and 48.4% of malignant lesions in T1-weighted images. On T2-weighted images, we found that 97% of benign lesions and 95.5% of malignant lesions showed hyperintense signal feature. In our study, a statistically significant difference was found between the isointense signal feature with adjacent muscle tissue and the condition of the masses being malignant (80%) on T1-weighted images, also between the hyperintense signal feature and the condition of the masses being benign (85.7%) on T1-weighted images (p = 0.002). When compared with the literature, this difference may be due to the number of the population, race, technique used and the differences in the stages of the masses. 17,18
As a general acceptance, 90% of malignant lesions are heterogeneous, although small lesions tend to be more homogeneous. The absence of heterogeneity is accepted as a reliable negative predictive indicator for malignancy. 18
Pang et al. reported that 68% of benign lesions showed a homogeneous signal intensity on T1-weighted images and 63% on T2-weighted images, while 39% of malignant lesions showed a homogeneous signal intensity on T1-weighted images and 11% on T2-weighted images and there was no statistical significance difference between both groups. 19 Totty et al. suggested that the majority of benign and malignant masses exhibit heterogeneous signal intensity and homogeneity differences do not help in the differentiation of benign from malignant. 20
Soler et al., in their study on 65 soft tissue masses, they reported that 42 masses showed homogeneous signal intensity on T1-weighted images and 43 masses heterogeneous signal intensity on T2-weighted images. These researchers also found that most of the benign tumors and non-tumor lesions were homogeneous in T1-weighted images (benign tumors, 64.2%; non-tumor lesions, 73.9%), 67.8% of benign tumors and 56.5% of non-tumor lesions exhibits heterogeneous signal intensity on T2-weighted images. They stated that malignant tumors showed heterogeneous signal intensity at a rate of 50% on T1-weighted images and 78.5% on T2-weighted images and there was no statistically significant difference between all three groups. 21
In our study, 67.6% of benign masses and 57.8% of malignant masses exhibited a homogeneous appearance on T1-weighted images. The relationship between homogeneity and benign and malignant masses in T1-weighted images was no statistically significant difference (p > 0.05). However, 61.7% of benign masses exhibited homogeneous and 67.6% of malignant masses showed heterogeneous signal intensity in T2-weighted images. A statistically significant difference was found between heterogeneity and malignancy in T2-weighted images (p = 0.005). This relationship is consistent with the literature. 10,13,14,19,22
Some researchers think that the presence of intralesional septa is useful in the differentiation of benign and malignant. 23,24 Hosono et al. have observed that liposarcomas generally show septation thicker than 2 mm and significantly enhancing while benign lipomas contain thinner septa. 25
In our study, we could not statistically evaluate the effect of septation and lobular contour in the detection of malignant and benign masses due to insufficient sample size.
Bongartz et al. reported that aggressive sarcomas may be surrounded by pseudocapsules and that desmoid tumors in the benign class may invade neighboring tissues. These researchers concluded that the margin features (smooth / well-circumscribed or irregular / poorly circumscribed) are not statistically significant in distinguishing between benign and malignant soft tissue masses in MRI. 26
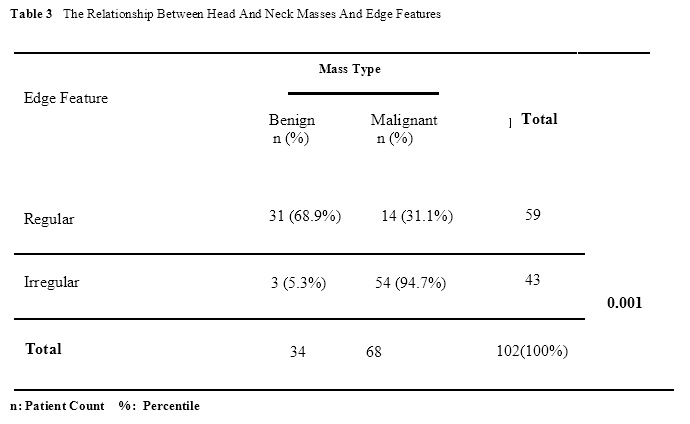
When we evaluate the margin properties of head and neck masses in MRI in our study; found that 68.9% of well-circumscribed lesions were benign and 94.7% of irregularly circumscribed lesions were malignant masses.
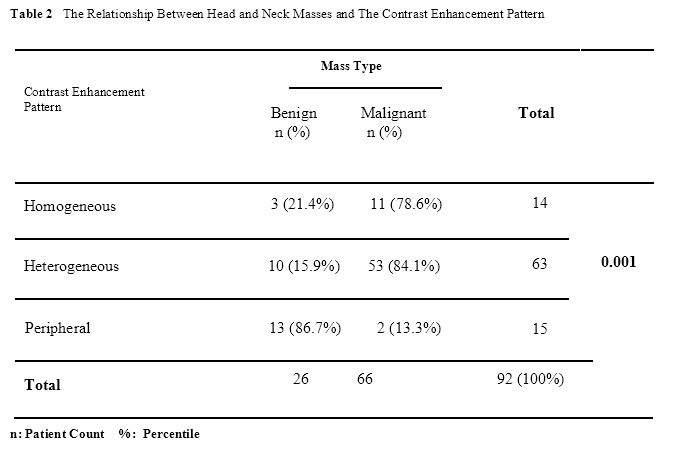
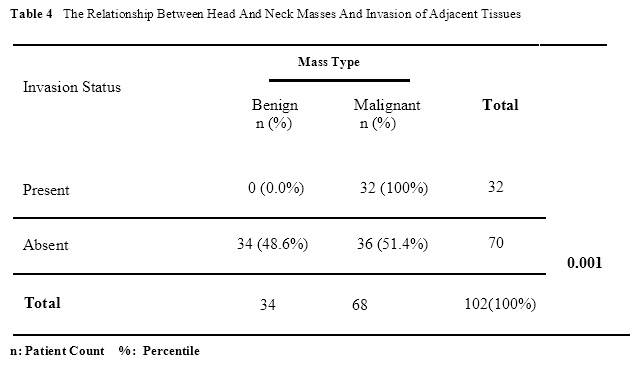
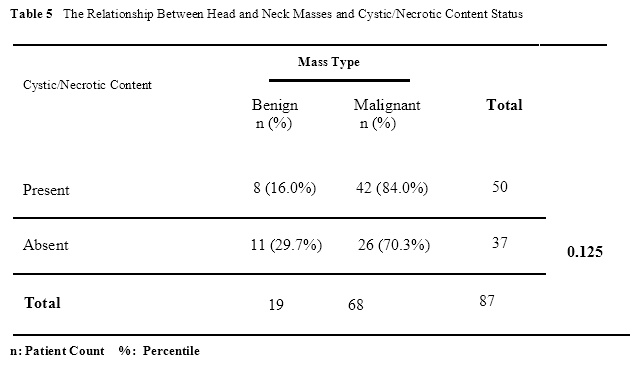
While invasion was not observed in adjacent tissues in any of the benign masses, invasion was observed in 47% of malignant masses. Accordingly, a statistically strong correlation was found between the benign - malign characteristics of head and neck masses, having irregular borders and showing invasion (p = 0.001). Masses with irregular borders and invasion were found to be malignant. This relationship is consistent with the literature. 10,20,21,26 The use of contrast material in MRI has an important place in the evaluation of pathologies belonging to the head - neck and other structures of the body. In addition, information about the distinction between tumor, muscle and edematous tissues, solid, cystic-necrotic components of the lesions and their spread can be obtained with contrast-enhanced MRI. 17,27 Benign and malignant tumors can show very different degrees of enhancement after contrast material injection in MRI. Although little vascularization and therefore low contrast were observed in some malignant lesions, increased vascularization and high contrast can be observed in some benign lesions. 14,28 Erlemann et al. reported that the enhancement ratio may be useful in the differentiation of benign and malignant soft tissue lesions. 29 When we evaluate the contrast enhancement pattern of head and neck masses in MRI in our study; heterogeneous enhancement was observed in 80% of the malignant masses which showed enhancement. A statistically significant relationship was found between head and neck malignant masses (80%) and heterogeneous enhancement in MRI (p = 0.001). This situation is consistent with the literature. 14,29 Chen et al., in their study on 118 masses (56 benign, 62 malignant), found that cystic-necrotic content was present in 9% of benign masses and 45.1% of malignant masses. They found the positive predictive value of necrosis observed in MRI to detect malignancy as 84.8% and its specificity as 90.9%.17 We found that 61.7% (n = 42) of malignant masses and 42.1% (n = 8) of benign masses in our study had a cystic-necrotic content. However, the relationship between cystic-necrotic content and malignancy was not statistically significant (p = 0.125). Compared with the literature, this difference may be due to the number of populations, race and the differences in the stages of the masses. 13,17
When we evaluate the relationship between bone involvement and head and neck masses in our study; bone involvement was detected in 18.7% of all lesions. 3 (8.8%) of the masses with bone involvement were benign and 16 (23.5%) were malignant. However, there was no relationship between bone involvement and malignancy (p = 0.072). In our study, the findings we obtained in terms of bone involvement in benign and malignant masses are compatible with the literature. 11,14
There are various studies in the literature investigating the characteristic features of benign and malignant masses with magnetic resonance imaging and obtaining different results. 7–18 De shepper et al., in the detection of malignancy in their study concluded that the margin feature of the lesion, its homogeneity on T2-weighted images, its intensity on T1-weighted images, degree of contrast and pattern are not statistically significant but low signal intensity in T2-weighted images, heterogeneous intensity on T1-weighted images and lesion diameter greater than 33 mm have high sensitivity in detecting malignancy. 30
Bequist et al. evaluated MRI appearance features (volume, edge features, signal intensity in T1 and T2-weighted sequences, bone involvement, necrosis and hemorrhage) of the 95 soft tissue masses (45 malignant and 50 benign) and concluded that the separation of benign or malignant masses could be detected by MRI at a rate of 90%.10 Crim et al. have reported that malignant lesions may exhibit well circumscribed and homogeneous appearance on MRI, therefore it is not reliable to distinguish benign from malignant with these parameters. 11 In some studies other than these, it has been suggested that the MRI appearance of soft tissue masses is non-specific. 7,9,20,31
Sundaram et al. stated that there is no reliable criterion for the differentiation of benign and malignant tumors after examined a total of 53 soft tissue masses (30 benign and 23 malignant) with MRI.9 Kransdoft et al. showed that specific diagnosis could be made only in 27 lesions (10 lipomas, 8 hemangiomas, 6 pigmented villonodular synovitis, 2 hematoma and 1 arteriovenous malformation) with specific MRI features of 112 lesions (85 benign and 27 malignant). 31
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}