Parkinson’s disease is a neurodegenerative disorder and is always accompanied by constipation [10]. Accumulating evidence suggests a direct impact of the gut microbiota and microbial metabolites on PD pathogenesis [11]. Both Meng-Fei Sun et al.[12] and Sampson et al.[13] demonstrated that gut microbiota not only affects the motor symptoms but also brain function in a PD model.
The concept of the “gut microbiota-brain axis” is well established and its dysregulation may lead to neurological diseases such as PD [14]. Microbiota seems to play an important role in the occurrence and development of neurological diseases and evidence indicates a potential bidirectional interaction between the gut microbiota and PD [15]. Studies show that the gut microbial composition of PD patients is different from HCs [16]. Changes in gut microbiota have also been observed in PD animal models with motor deficits and neuroinflammation [17].
Gastrointestinal dysfunction is one of the most common non-motor symptoms in PD, especially constipation [18]. Studies suggest that neurotoxic substances with prion-like properties may be improperly folded.α-Syn a typical pathogenic agent for PD, is transported from the gastrointestinal tract to the central nervous system during the early stages of PD [19].
Sampson et al.[13] showed that gut dysbiosis leads to an altered ratio of short-chain fatty acids (SCFA). SCFA modulates the activity of the ENS and increases gastrointestinal motility [20], especially butyrate, and alters the microglial signaling in the brain leading to disease development and the appearance of PD-associated motor symptoms [21]. Hence, the altered concentrations of SCFA might contribute to the gastrointestinal dysmotility in PD. In recent years, an increasing number of studies have shown that the levels of certain gut microbiota differ between PD patients and HCs [22].
FMT is a well-established treatment for the reconstruction of gut microbiota [23] and has been proposed as a therapeutic option for functional gastrointestinal disease [8]. It can repair the disruption of the normal microbial communities for the efficient treatment of metabolic disorders [24]. Dae-Wook Kang et al. [25] found that microbiota transfer therapy led to significant improvements in both GI- and ASD-related symptoms, and the improvements were sustained for at least 8 weeks after the treatment. Sampson et al. [13] found that fecal microbiota transplantation from PD patients, compared to microbiota from HCs, exacerbates the α-Syn mediated motor dysfunction in ASO mice, demonstrating that gut microbiota can influence brain function in PD.
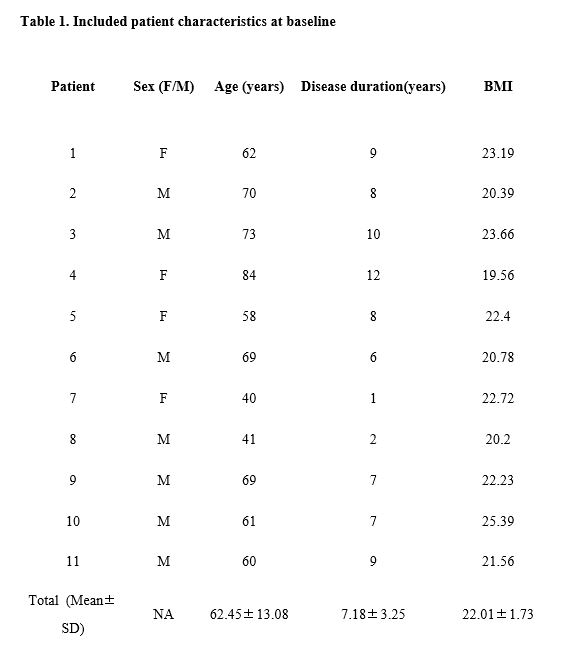
At our center, FMT treatment has been used for PD patients with gastrointestinal dysfunction since 2018. In 2019, Hongli et al. [9] reported successful FMT treatment in a PD patient with constipation, which encouraged us to summarize and analyses the FMT-treated patients from the last two years. In our study, remission of the constipation symptoms was observed in all patients, which might be related to increased microbial abundance. Here we report alterations in the gut microbiota composition that reproduce some of these previously reported findings among PD patients, before and after FMT, and HCs using the 16S rDNA sequencing analysis. We observed a decrease in the community abundance of fecal microbiota and the microbial diversity was lower in before-FMT PD patients compared to the after-FMT and HCs; all differences were statistically significant.
The abundance of Blautia and Lachnospiraceae (Phylum: Firmicutes) was significantly increased in the after-FMT groups comparing to the before-FMT PD patients. We observed a significantly increased abundance of Bacteroides (phylum: Bacteroidetes) and a significantly reduced abundance of Faecalibacterium (phylum: Firmicutes) among the PD patients, before and after FMT, compared to the HCs. Faecalibacterium prausnitzii is the representative species of Faecalibacterium that produce butyrate and is a beneficial gut bacterium with anti-inflammatory properties; its levels are reduced in PD patients [26]. The significant reduction in the abundance of Faecalibacterium in PD patients before FMT in our study is consistent with the previous study [26]. Besides, Keshavarzian et al. found Bacteroidetes to be positively correlated with the PD duration[15].
Our results were similar to theirs, however, we observed no correlation between the PD duration and the abundance of Bacteroidetes or Firmicutes. Further studies are required due to the limited number of cases.
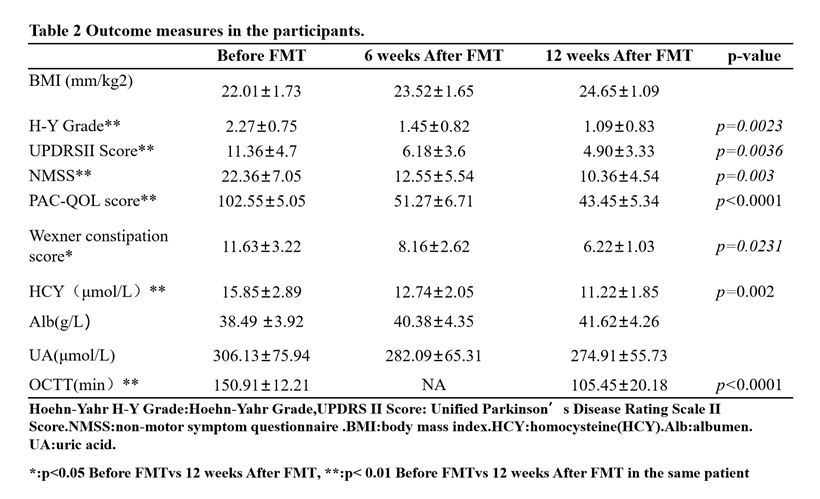
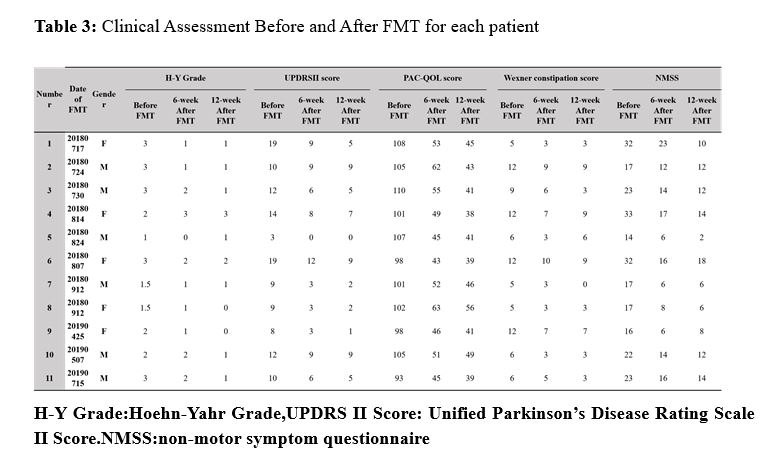
Similar to the study by Keshavarzian et al. [17], we also observed an increased abundance in the Enterobacteriaceae (phylum: Proteobacteria) in PD patients before FMT. Scheperjans et al. [16] observed that the relative abundance of Enterobacteriaceae in PD patients was positively correlated with postural instability and gait difficulty. Similarly, the abundance of Escherichia−Shigella (Family: Enterobacteriaceae) also gradually decreased in the three after-FMT groups compared to the before-FMT PD patients. Similarly, we observed that postural instability and gait difficulty improved and that the H-Y grade, UPDRS, and NMSS of PD patients decreased significantly after FMT. Therefore, a correlation may exist between the changes of the abundance of Escherichia−Shigella and the clinical symptoms, and that FMT may have a positive impact on the relief of clinical symptoms in PD patients.
In addition, we also observed a decreased abundance of Blautia and Prevotella (all affiliated with Firmicutes phylum), butyric acid-producing bacteria, in PD patients before FMT. Our results are similar to those by Keshavarzian et al [12]. Recent studies have shown that bacteria that can produce SCFA, to be reduced in PD [16]. SCFA such as butyrate modulates the activity of the ENS and thereby increase the gastrointestinal motility [27]. Hence, the altered concentrations of SCFA might contribute to gastrointestinal dysmotility in PD. In our study, the remission constipation symptoms were observed in all PD patients after FMT and the benefits continued for at least 12 weeks. Thus, it appears that FMT treatment might lead to significant improvements in GI symptoms in PD patients. Further studies are needed to further clarify this.
Gut microbiota and their metabolic products are potential candidates that could initiate a process, eventually leading to Lewy body formation in the ENS [28]. As PD advances clinically, dysfunction of ENS (dysautonomia) increases which leads to slowing of GI motility, which in turn predisposes the PD patients to small intestinal bacterial overgrowth (SIBO) [29].
The role of SIBO has been studied by Fasano et al. [30], who showed that the prevalence of SIBO is higher in PD patients than the HCs. In our study, SIBO correction with the FMT (after 12 weeks) resulted in improvement of GI symptoms along with improvement in the motor fluctuations (P < 0.04). This suggests that FMT may be able to reverse the phage-mediated dysbiosis of the PD gut, although further studies are required to confirm this assertion.
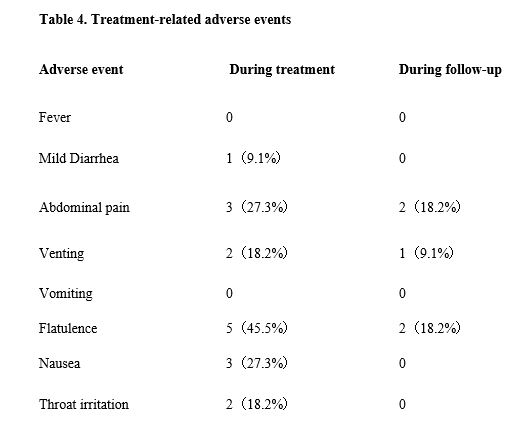
FMT is considered to be a safe treatment. Previous studies show that almost all of the common adverse events, such as venting, abdominal pain, bloating, and diarrhea, disappeared after 12 weeks [8]. In our study, we did not observe any adverse events, such as fever, abdominal pain, hypoxia, paroxysmal atrial fibrillation (PAF), transplant-related lower gastrointestinal bleeding, cholestasis, liver damage. Xiaofei Qi et al [31] reported that a patient treated with FMT for sterile refractory intestinal acute graft-versus-host disease experienced thrombocytopenia after FMT. We did not observe this in any of our 11 patients.
Based on our results, FMT is a good choice for PD treatment with gastrointestinal symptoms; however, its effectiveness and safety requires further evaluation. In order to evaluate the effectiveness and safety of FMT in the treatment of PD accurately, a larger sample study is required in the future.
This tentative study may open a new avenue to study the mechanism of the microbe-gut-brain axis and the biological treatment of PD. The current use of FMT to treat PD is beginning and it has inspired us to further our understanding of FMT in treating neurological diseases.
In conclusion, our patients demonstrated efficient reliving of PD constipation by FMT and its positive impact on clinical characteristics. The changes before and after FMT suggest the potential for a more targeted and specific FMT therapy in PD. FMT can be used for the treatment of PD with gastrointestinal symptoms, but its effectiveness and safety requires further evaluation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}