Feeding difficulty is a long-standing problem. Its increased incidence is probably related to the increased survival rate of preterm birth or infants with multiple malformations[8]. However, the overall attention is dreadfully insufficient. Generally classified as neonatal encephalopathy, treatment for feeding difficulty usually relies on tube feeding such as nasogastric tube (NGT) and gastrostomy tube placement (G-tube). Yet little has been known for its potential genetic causes, feeding difficulty might be the alert of rare genetic disease, causing high rates of misdiagnosis and delayed intervention. In this study, we tried to analyze its different clinical manifestations and reveal the genetic causes of feeding difficulty of unknown etiology.
Phenotypic evaluation
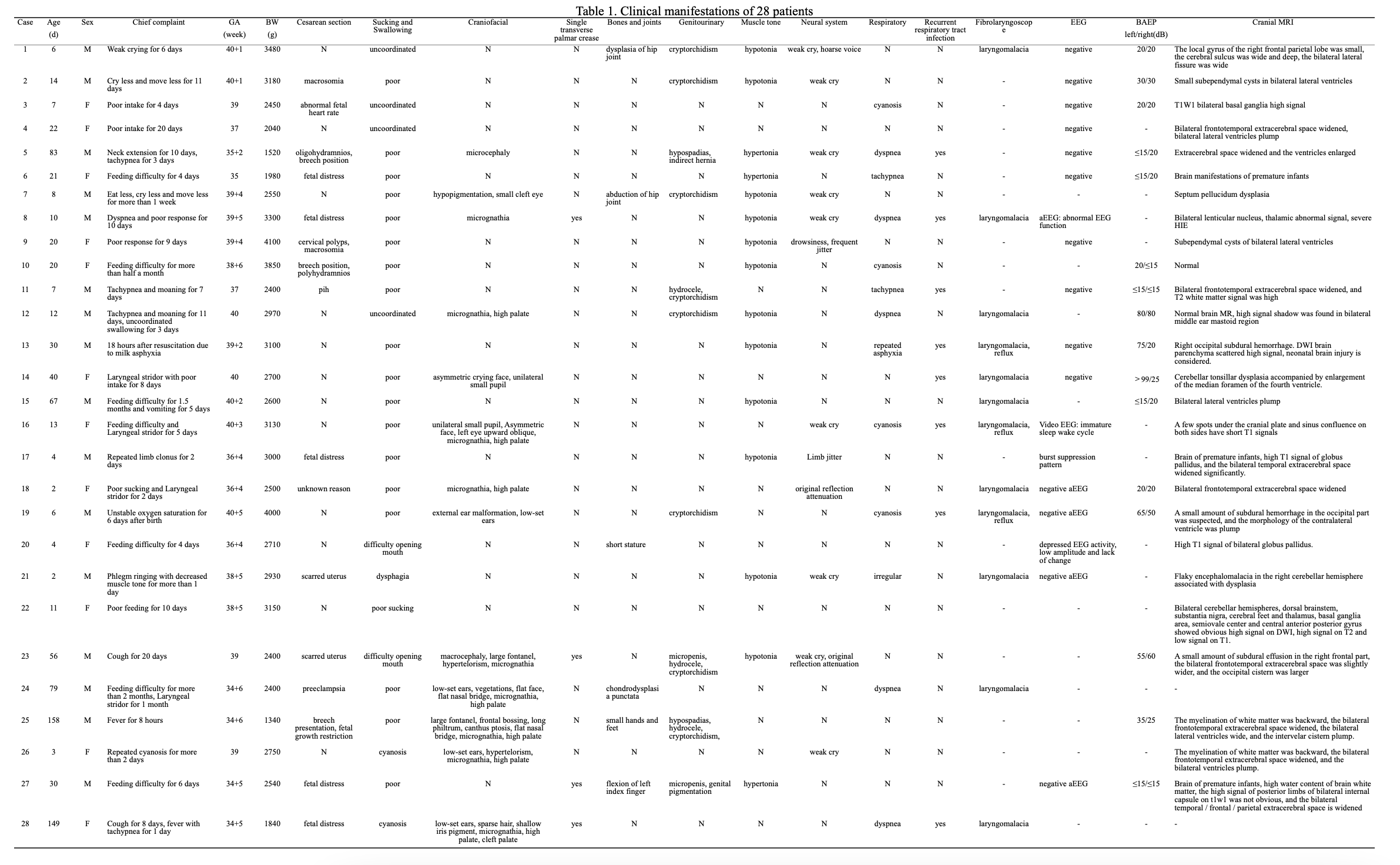
In our study, only half of the patients came with the chief complaint about feeding problem, and only 3 came within one week old. Some parents had awfully poor awareness about feeding difficulty and its consequences. Patient No.25 and No.28 were admitted at 158 and 149 days of age, without mentioning feeding problems in the chief complaint, and their weight fell far below the third percentile of the growth chart.
32.1% of patients were SGA, with the same proportion of cesarean section due to fetal problems, suggesting that their feeding difficulty might be relevant with abnormal intrauterine development. High rates of patients were complicated with multiple malformations, with or without muscle tone and neurological abnormalities. However, the vast majority of patients lack the classic phenotype to diagnose, usually generally classified as chromosome disease or encephalopathy by clinicians.
Clinical evaluation are essential for identifying feeding difficulty. Nevertheless, an agreement on the gold standard for pediatric dysphagia assessment has not been reached in the literature[4]. Videofluoroscopic swallow study (VFSS) and fiberoptic endoscopic evaluation of swallow (FEES) are the most commonly used instrumental assessments in pediatric dysphagia. Fibrolaryngoscope might discover laryngomalacia and allow the detection of structural and physiological swallowing impairments without radioactive exposure or risk of contrast medium aspiration. In our cohort, laryngomalacia was also found at a high rate (42.9%), but often without obvious stridor on clinical presentation. We cannot judge how much its laryngomalacia affected the feeding difficulties. But the presence of reflux was confirmed by laryngoscopy in 3 cases who presented with recurrent cyanosis and respiratory infections.
Feeding, sucking and swallowing needs multi-system collaboration, whereas central neurological system drive is critical. Neurological system was assessed by EEG/aEEG, BAEP and cranial MRI from different aspects.
The amplitude-integrated electroencephalogram (aEEG) can be used for long-term monitoring of brain function, mainly after perinatal asphyxia and seizure detection[9]. Research shows aEEG background is correlated with cerebral white matter damage and neurodevelopmental outcome[10]. In our study, 4 out of 18 patients had positive findings in EEG/aEEG. Burst suppression pattern was detected on Patient No. 17 who was identified with KCNQ2 gene variant and finally diagnosed Early myoclonic encephalopathy(EME). The other 3 patients had monitored abnormal function or depressed activity.
There was a high percentage(43.8%) of neurological hearing impairment among the 16 children who underwent brainstem auditory evoked potentials (BAEP). BAEP abnormality is considered to be an early indicator for brain insult[11]. In our study, the positive rate of BAEP was much higher than that of aEEG. This means that brain injury are likely to be present in a significant proportion of patients with feeding difficulty.
There is no doubt about the importance of imaging in the evaluation of neurological development and lesions. And astonishingly, 96.2% of patients had positive findings in cranial MRI, with a significant fraction(44%) presenting widening extracerebral space or enlarged ventricles, indicating that feeding difficulty might be associated with cerebral atrophy and white matter loss[12] which we would explore further in ongoing research.
Genetic manifestations
There are about 7000 rare diseases with genetic causes, leading to nearly 80% of all cases usually with misrepresented symptoms leading to incorrect diagnosis[13]. Whole-exome sequencing (WES) contains an estimated 85% of heritable Mendelian disease-causing mutations[14], yielding a diagnosis of the underlying genetic cause in 25–35% of children with an unexplained presumed genetic disorder or fetal structural anomalies[15].
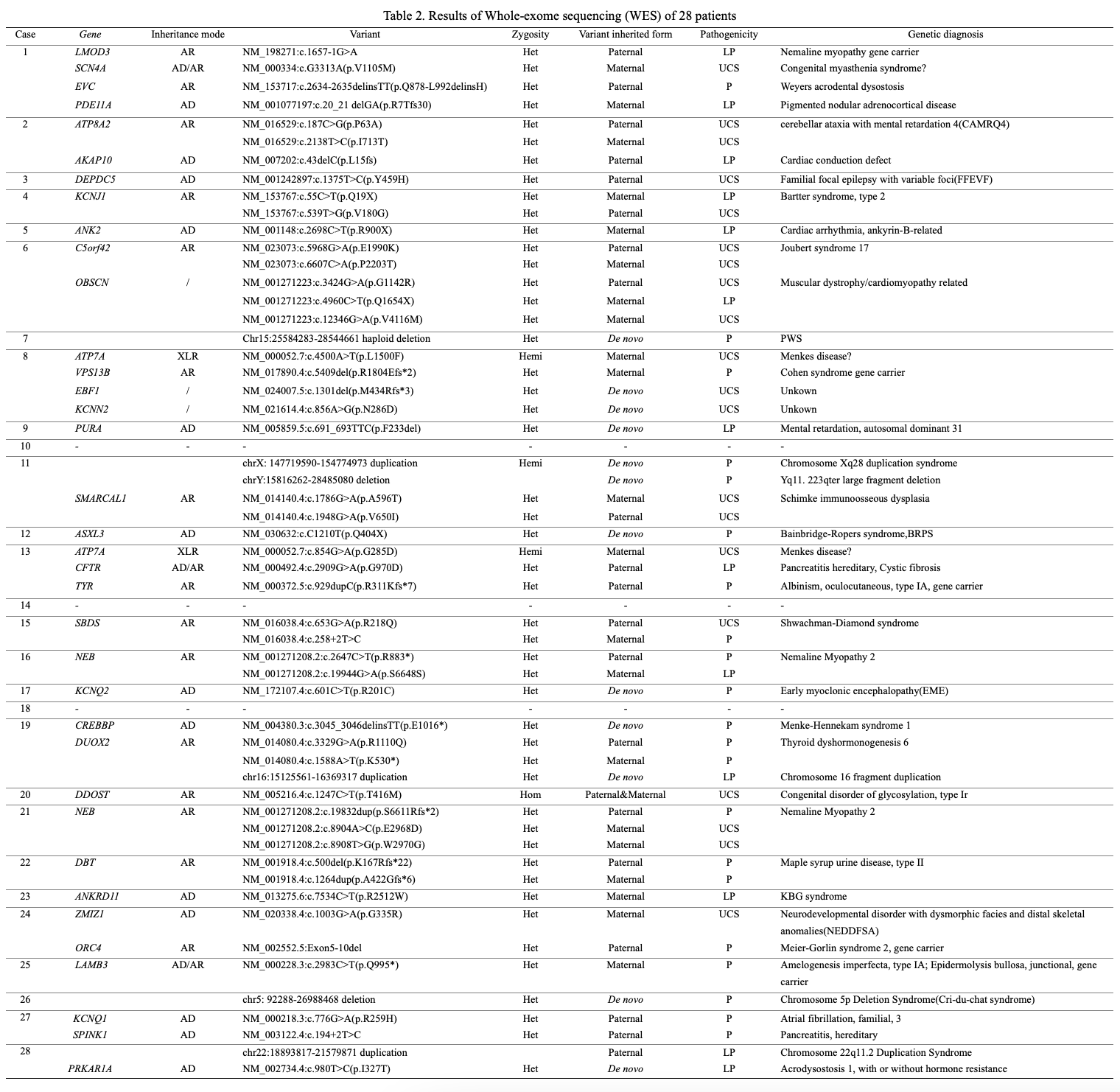
In this study, we found that rare genetic diseases underlie a significant proportion of infants presenting with feeding difficulty of unknown etiology. 89.3% of patients in our study had positive findings in WES with 50% genetically diagnosed and 28.6% suspected diagnosed. The genotype spectrum covers a wide range mainly composed of rare diseases.
Clinical presentation is incomplete for part of patients. Patient No.4 was admitted with chief complaint “poor intake for 20 days”, found with hyperkalemia, hyponatremia, hyperglycemia during hospitalization, and was misdiagnosed with pseudohypoaldosteronism. Compound heterozygous variants of KCNJ1 gene were identified by WES leading to final diagnosis of Bartter syndrome, type 2, whereas the typical feature should be opposite——hypokalemia. Studies found mutations in the potassium channel ROMK gene (KCNJ1) tend to develop transient hyperkalaemia in the first month of life[16]. Thus, the results of WES rescued the wrong direction of treatment. Patient No.12 presented with uncoordinated swallowing, micrognathia, high palate and hypotonia, clinical diagnosis was considered as Robin sequence. De novo heterozygous variant of ASXL3 gene was identified and made final diagnosis of Bainbridge-Ropers syndrome[17]. As the ASXL3 variant identified in the proband was not identified in either parent, the risk to sibs was presumed to be low, but genetic counseling are still needed.[18]
Especially for young infants whose clinical characteristics may be atypical and drift with disease progression, WES could even identify the causative variant in single gene disorders prior to clinical manifestation[19]. Patient No.15 presented with feeding difficulty, failure to thrive and hypotonia, compound heterozygous variants of SBDS gene were identified and Shwachman-Diamond syndrome was diagnosed. During later follow-up, the patient gradually developed typical clinical manifestations of thrombocytopenia and neutropenia[20]. Some of our patients were incidentally found with other genetic diseases that had not yet appeared clinical symptoms, or to be carriers of recessive genetic diseases, suggesting more attention should be paid for those areas in the future.
Patient No.16 and No.21 were both genetically diagnosed Nemaline Myopathy 2 with compound heterozygous variants of NEB gene. Due to the unremarkable muscle enzymes and electromyogram, the diagnosis of nemaline myopathies rely on histological features on skeletal muscle biopsy and genetic correlations with the contribution of muscle MRI[21]. However, biopsies were invasive and limited to diagnosis of muscle disorders, making genetic examination more acceptable by parents.
Clinical phenotypes of patients with rare genetic diseases are diverse. In a subset of patients in this study, multiple genetic abnormalities, even copy number variations (CNVs) were found. The clinical presentation of patient No.19 was multiple malformations, hypothyroidism, feeding difficultiy and recurrent respiratory infections. Heterozygous variant of CREBBP gene and compound heterozygous variants of DUOX2 gene were identified, besides, significant increased intensity of signal was captured in chromosome 16 and verified by chromosomal microarray analysis(CMA), leading to the diagnosis of this patient as Menke-Hennekam syndrome 1, Thyroid dyshormonogenesis 6 and Chromosome 16 fragment duplication simultaneously[22].
The suspected diagnosed 8 patients had found variants of unknown significance (VUS) with corresponding clinical manifestations. Patient No.8 and No.13 shared similar history of asphyxia and hypotonia after feeding, followed with manifestations of HIE on the MRI. Variant of maternal ATP7A gene were identified in both of them and Menkes disease was suspected. Along with the improvement of genetic research, the current VUS may get more studied to clarify its clinical significance. Further follow-up and research are needed.
Limitations
Our study was limited by its design. The criteria for judging feeding difficulty came from previous articles and were subjective to some extent due to the lack of quantitative indicators. Feeding difficulties caused by specific etiology such as severe cleft palate were excluded in this study. Premature infants within 34 weeks of gestation were excluded due to a history of mechanical ventilation or nasogastric tube insertion after birth. For other diseases such as spinal muscular atrophy (SMA) and PWS with typical clinical manifestations are not suitable for definite diagnosis with WES method and were excluded in this study. Some patients were unable to complete relevant examinations due to their critical condition, resulting in biased results.
Generalisability
In spite of the limitations, this study has good generalisability and is suitable for implementation. The genetic causes of feeding difficulties are not limited to the results of the cases in this study. The disease spectrum of feeding difficulties may be gradually enriched in further studies.
In conclusion, Feeding difficulty might be part of the phenotype spectrum of rare genetic diseases that deserve attention and in-depth exploration. WES is of vital importance for the diagnostic process especially for young infants with misrepresented symptoms. We therefore recommend WES along with neurological assessment(cranial MRI, BAEP and aEEG) for patients with feeding difficulty of unknown etiology. And to reduce financial pressure, we also appeal for establishing a targeted panel for the relevant genetic spectrum of feeding difficulty.
{kind=link}
{kind=link}