Surgical intervention for spontaneous pneumothorax is recommended for blebs identified on chest CT-scans, especially in cases of recurrence or in patients who might engage in “high-risk situations”, such as flying, scuba diving or hiking, where access to medical care may not be immediately available. Surgery is typically performed through VATS approach that includes bleb resection and pleurodesis, usually mechanical, aimed at preventing lung collapse and tension pneumothorax in case of a recurrence by creating adhesions between the parietal and visceral pleura.3,4
Mechanical pleurodesis is frequently accomplished by using the Bovie scratch pad, an off-label application (fig.1). It is intended to clean the electro-cautery tip when needed; however, its universal presence, low cost and ease of use have led many thoracic surgeons to use them for pleurodesis. Its use has been reported by others and described in the training manual of the Society of Thoracic Surgery (STS).5 We have successfully carried out this practice for many years without any adverse effects.
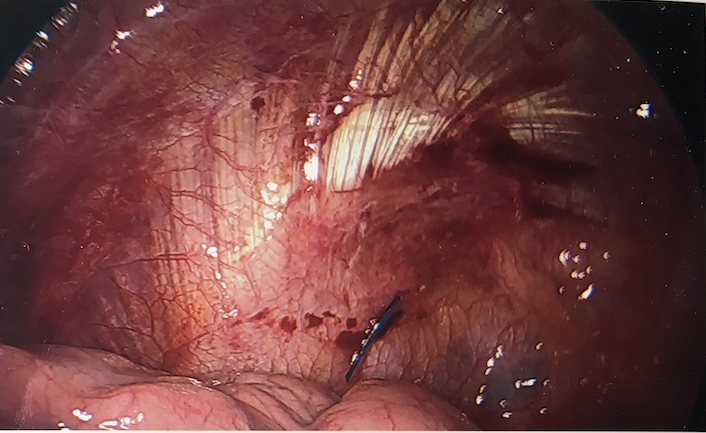
The instrument count at the conclusion of the operation was correct, as the counted item was the pad itself and not the marker. The radiological report of the immediate portable postop chest x-ray did not mention the FB, although in retrospect it can be visualized. The marker was in close proximity to the parenchymal staple line and thought to be part of it (fig.2). It became more apparent when an apical pneumothorax, following chest tube removal on day three, moved the staple line away from the marker (fig.3). Our index of suspicion was high that the abnormality seen was the marker but could not be absolutely certain, as the pad had been already discarded as one might expect.
It was formerly customary for us to cut the scratch pad in half for easier introduction through the small VATS incision. This perhaps “weakened” the product and permitted the marker to separate from the pad, as it is difficult to remove it from an intact and uncut pad. One thought was to remove the marker off the cut pad prior to its insertion into the chest. This perhaps may create a worse problem of retaining an unmarked pad that cannot be detected radiographically in case of an incorrect count. It is also against our and probably many others institutional policies of minimizing use of unmarked instruments and devices.
Our current practice is to use a full (uncut) folded pad and continue to perform pleurodesis per STS guidelines, unless further studies corroborate the work by Min et al. showing no difference in recurrence rates in patients with and without pleurodesis.6 A conscious effort is also made at the end of each case to specifically identify the marker within the scratch pad at time of instrument count.
{kind=link}