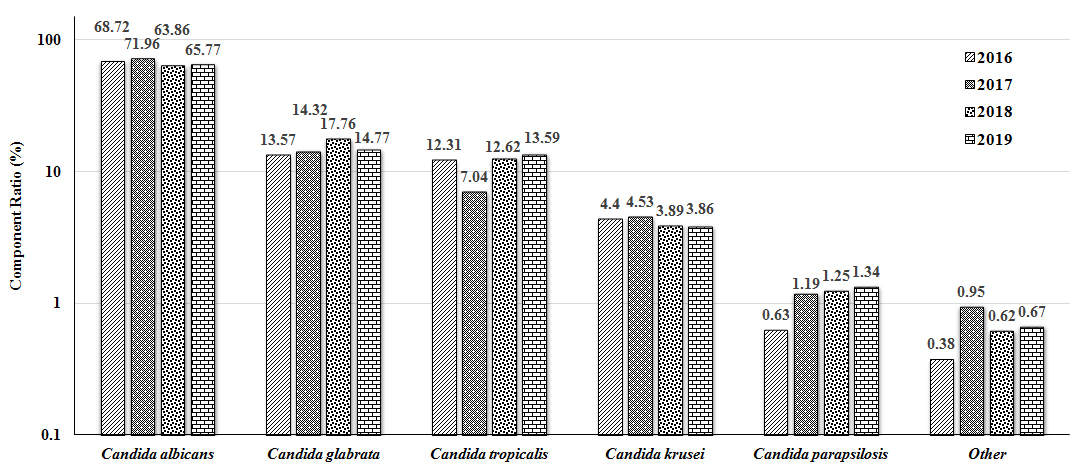
Isolation of Candida
The strain distribution of various types of Candida detected in the hospital from 2016 to 2019 was analyzed. As shown in Fig. 1, totally 2872 strains of Candida were detected. After the Cochran Q test, the composition ratio of various Candida species in each year showed statistical significance (Q = 1101.094–1904.945; all P < 0.001). For each year, Candida albicans was the major strain, accounting for more than 60% (up to 71.96% in 2017), followed by Candida glabrata, accounting for about 15%, and Candida tropicalis ranked the third, with no significant change in the proportion between 2016, 2018 and 2019 (all around 13%, which fell to 7.04% in 2017). In addition, the comparison of the composition ratio of Candida over these four years also had statistical differences (χ2 = 33.344; P = 0.004). However, the composition ratio of each kind of Candida was compared between these four years. Our results showed statistical significant only for Candida albicans (χ2 = 12.620; P = 0.006) and Candida tropicalis (χ2 = 20.410; P < 0.001), and the proportion of Candida albicans exhibited a gradual decrease (χ2 = 4.558; P = 0.033) over these years. However, there were no differences in the detection over these years for Candida glabrata, Candida tropicalis, and Candida krusei (Additional file 1:Fig. S1).
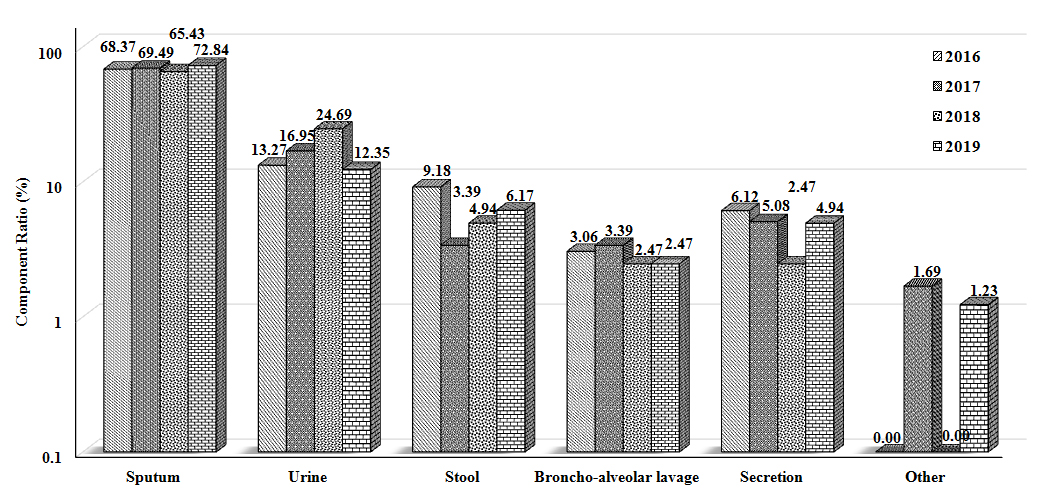
Sources of Candida tropicalis samples
The Candida tropicalis samples detected over 2016–2019 were classified according to the sample sources, and the composition ratios were also analyzed. Our results showed that significant differences were observed in the proportion of samples from which Candida tropicalis was detected in each year (Q = 123.949–194.898; P < 0.001) (Fig. 2). Moreover, for each year, the major sample source was the airway secretion (more than 65%), followed by the mid-range urine (12%-25%). Although there was no statistical difference in the composition ratio of the source for Candida tropicalis samples for these four years (χ2 = 14.858; P = 0.399), the proportion of urine samples detected with Candida tropicalis was statistically different between these years (χ2 = 9.387; P = 0.025). Furthermore, our results from the trend test showed that, except for the proportion in the stool samples (χ2 = 3.550; P = 0.060), the proportions in the airway secretions and urine samples were increased over the years, which were decreased in the remaining samples year by year (all P < 0.050) (Additional file 2:Fig. S2).
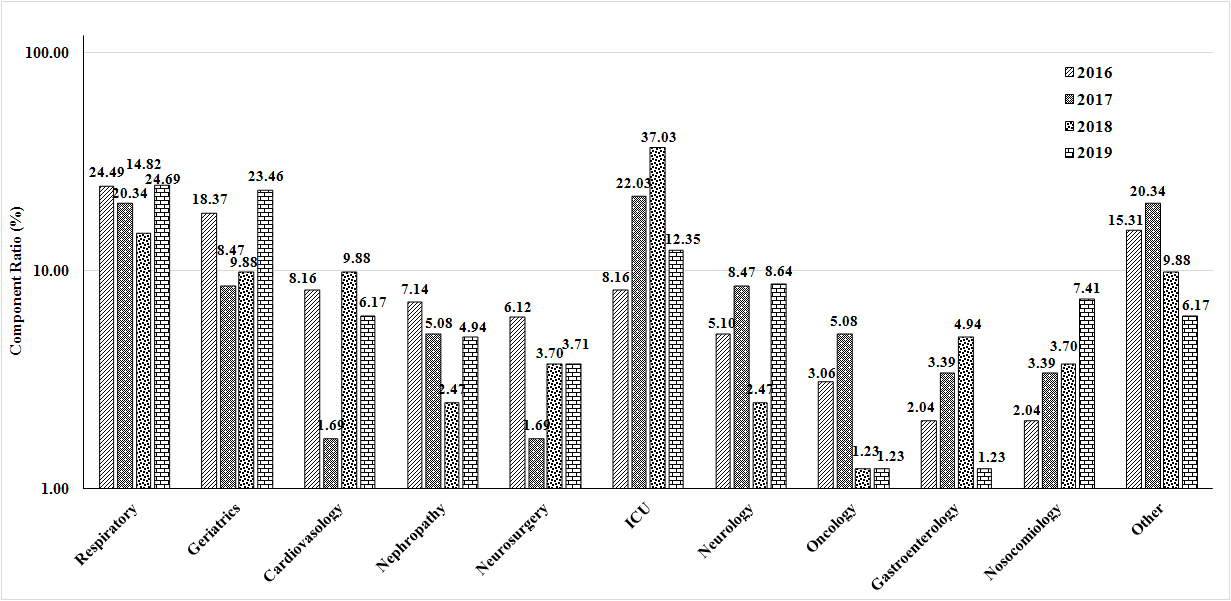
Department distribution of Candida tropicalis
The department sources of Candida tropicalis in 2016–2019 were analyzed. Our results showed that, from 2016 to 2019, significant differences were observed in the distribution of Candida tropicalis in these departments (Q = 40.746–92.691; all P < 0.001). The departments with relatively high detection rates included the Departments of Respiratory Medicine, ICU, and Geriatrics (Fig. 3). Moreover, among the proportions of Candida tropicalis detected in different departments, the detection rates of Candida tropicalis in the Department of Respiratory Medicine were more than 20% in 2016, 2017 and 2019, which fell to 14.82% in 2018. Furthermore, the amount of Candida tropicalis detected in the ICU had been increasing year by year, from 8.16% in 2016 to 37.03% in 2018, which was decreased to 12.35% in 2019. The proportions of Candida tropicalis detected in the Department of Geriatrics were higher in 2016 (18.37%) and 2019 (23.46%), while lower in 2017 and 2018 (about 9%). The composition ratio of Candida tropicalis detected in different departments between four years suggested statistically significant differences (χ2 = 58.045; P = 0.002). However, for the comparison of the Candida tropicalis amount detected in each department between four years, statistically significant differences were observed in the amount of Candida tropicalis in the Department of Geriatrics (χ2 = 8.623; P = 0.035) and ICU (χ2 = 27.148; P < 0.001) (Additional file 3:Fig. S3).
Resistance of Candida tropicalis to antifungal drugs
The resistance of Candida tropicalis to azoles such as fluconazole, itraconazole and voriconazole, from 2016 to 2019, was analyzed. Our results showed that Candida tropicalis had high resistance rates to fluconazole, itraconazole, and voriconazole, with even the cross-resistance phenomenon. In 2018, the resistance rate of Candida tropicalis to fluconazole was up to 39.2%. There was no statistically significant differences in the resistance rates of Candida tropicalis to azole antifungal drugs over these four years (χ2 = 1.156; P = 0.979).
Relative mRNA expression levels of ERG11 and UPC2 in Candida tropicalis
In order to further study the resistance-related genes of Candida tropicalis, the mRNA expression levels of ERG11 and UPC2 were detected with the quantitative real-time PCR. Our results showed that the data of the relative mRNA expression levels of ERG11 and UPC2 genes in the Candida tropicalis from the fluconazole-resistant groups (27/30 strains fully resistant to fluconazole, itraconazole, and voriconazole) and fluconazole-sensitive groups were in the normal distribution. Based on the paired sample t-test, the relative mRNA expression levels of ERG11 in the drug-resistant group was 1.579 ± 0.896, while the relative mRNA expression of ERG11 in the sensitive group was 0.483 ± 0.259, with statistical significance (t = 4.511; P < 0.001) (Fig. 4A). On the other hand, the relative mRNA expression levels of UPC2 in the resistant group was 1.400 ± 0.919, while the relative mRNA expression levels of UPC2 in the sensitive group was 0.448 ± 0.272, with statistically significant difference (t = 3.970; P < 0.001) (Fig. 4B). These results suggest that the resistance of Candida tropicalis to fluconazole is related to the expression levels of ERG11 and UPC2.
Correlation analysis of UPC2 and ERG11 mRNA expression in Candida tropicalis
The mRNA expression levels of resistance-related genes (i.e., the ERG11 and UPC2) in Candida tropicalis were detected, and the correlation between the gene expression levels was further analyzed. Our results from the Spearman correlation analysis showed that there was no liner correlation between the expression levels of UPC2 and ERG11 in the sensitive group (r = − 0.074; P = 0.757) (Fig. 5A). However, the UPC2 and ERG11 expression levels were positively correlated in the drug resistance group (r = 0.571; P = 0.001) (Fig. 5B). These results suggest that the over-expression of fluconazole-resistant ERG11 in Candida tropicalis may be related to the regulation of UPC2.
{kind=link}
{kind=link}
{kind=link}