In this study, we overall performed 409 MDW measurements during clinical-laboratory monitoring of 87 hospitalized COVID-19 patients, ranging 1-18 MDW detections/patient (median 4 time-points per patient).
MDW shows significant correlations with inflammatory markers in COVID-19 patients
First, based on the laboratory dataset available for our cohort of 87 COVID-19 patients with at least one MDW measurement, we performed repeated measures correlation analysis (rmcorr) to compare MDW with main inflammatory markers frequently tested in this setting, as part of routine laboratory monitoring. As shown in Figure 1, a significant correlation with C-reactive protein (CRP) (n=69 patients, p<0.001), fibrinogen (n=84, p<0.001) and ferritin (n=63, p<0.01) has clearly emerged, but not with other common biomarkers (data not shown), such as lactate dehydrogenase (LDH) (n=84, p=0.70), D-dimer (n=35, p=0.18) and interleukine-6 (IL-6) (n=65, p=0.31). In line with another report [19], here we found that procalcitonin (PCT) resulted negative (<0.5 ng/mL) in the majority of the tests performed (135/228), thus showing only a limited impact in the clinical monitoring of COVID-19 patients, and hampering the execution of significant comparisons. However, it could also be the case that PCT may better reflect the development of overcoming severe opportunistic infections (i.e. bacterial sepsis), which can complicate the clinical course of severe COVID-19 patients undergoing long-term hospitalizations [20]. Of note, we also observed a good association between MDW values and body temperatures (p<0.05), further indicating that high MDW values may be associated with inflammatory syndromes, often including fever (body temperature >37°C).
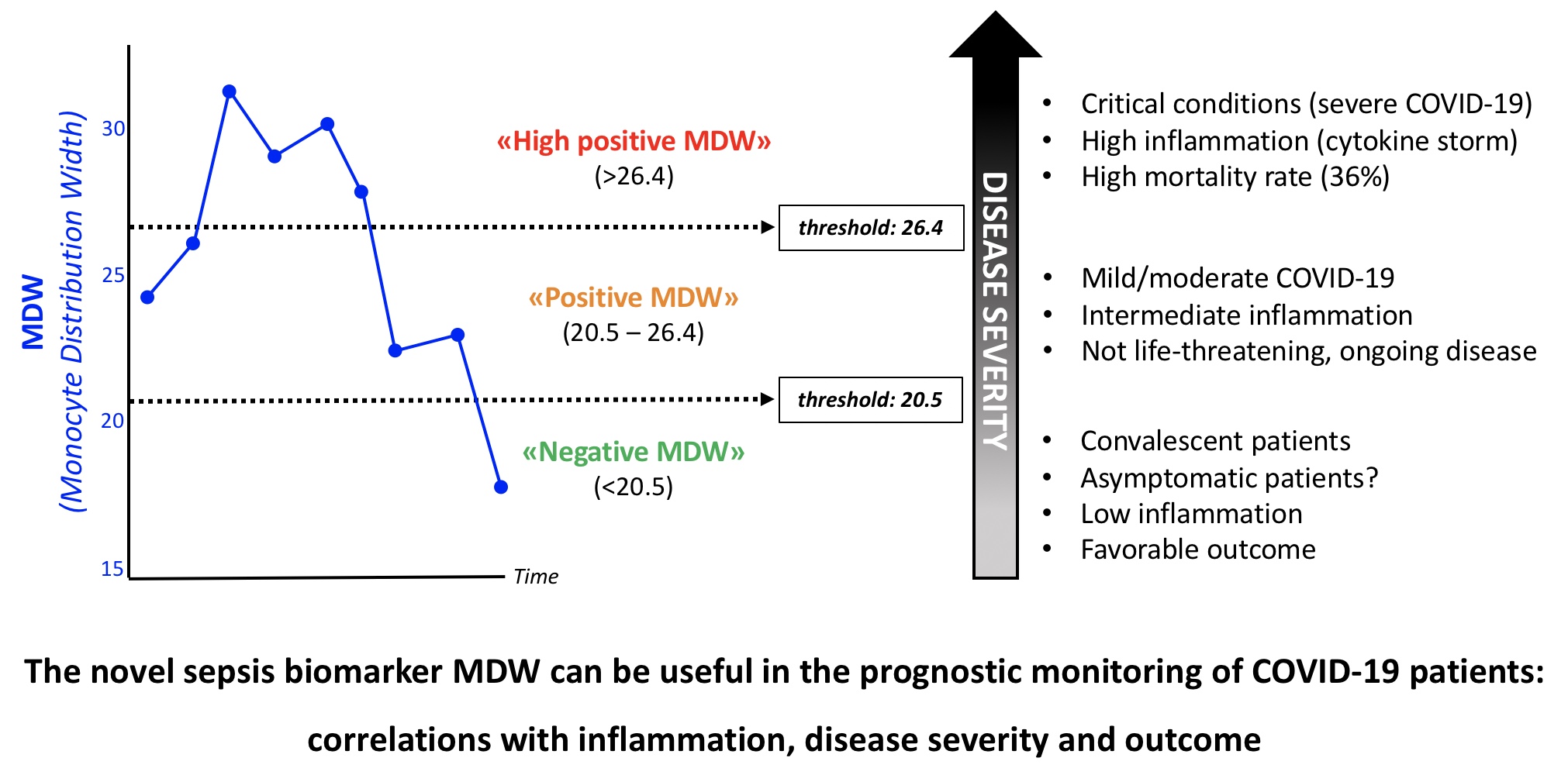
MDW is associated with the clinical outcome of COVID-19 patients
In our cohort, we recorded 71 (81.6%) favorable cases and 16 (18.4%) fatal outcomes. By applying Mann-Whitney test for independent values, we found a significant correlation (p<0.001) between the last value of MDW detected in each patient (n=87), and the final clinical outcome (survival/discharge vs death). Indeed, by considering the group of 71 surviving patients, the median ‘last MDW value’ was 19.6, while this median rose up to 26.1 in the group of 16 patients with unfavorable outcome (Figure 2A-B). Such observation prompted us to further investigate whether MDW could provide prognostic information in this setting. Therefore, by performing ROC curve analysis (Figure 2C), we identified a MDW value of 26.4 as best cut-off to assess the probability of fatal evolution during the disease course in our cohort of COVID-19 patients (n=87). This analysis provided a promising area under the curve (AUC) of 0.76 (95% CI: 0.66-0.87; sensitivity, 0.75; specificity, 0.70). In details, among 33 out of 87 patients showing at least one MDW value >26.4, 12 cases had fatal outcome, meaning that high MDW values are associated with a mortality rate (absolute risk) »35%. Of note, almost all the remaining 21 patients, who survived despite high MDW levels, also developed a critical phase characterized by a hyper-inflammatory condition, which however was well controlled and, eventually, had a favorable clinical course, often associated with a consistent decline of MDW values. On the other hand, only 4 out of 54 patients (<10%) died although showing MDW values always lower than 26.4 (Negative Predictive Value, NPV=0.93). Putting together these data, by applying Yates’ corrected Chi-square test, we detected a significant association (p<0.01) between MDW values and final clinical outcomes, also showing remarkable risks of fatal evolution when MDW values were above 26.4 (RR=4.91, 95% CI: 1.73-13.96; OR=7.14, 95% CI: 2.06-24.71; RR and OR p-values=0.001).
MDW correlates with clinical severity and disease course in COVID-19 patients
In order to evaluate whether MDW values could be associated with different levels of disease severity (putatively driven by detrimental inflammation) during COVID-19 clinical course, we compared MDW values with a common score clinically used to monitor critical patients, i.e. ‘sequential organ failure assessment’ (SOFA score), which was periodically calculated in our COVID-19 patients, basically after each execution of blood gas analysis. To this aim, we were able to identify a group of 16 patients (12 surviving and 4 deceased), showing temporal associations (<12h) between MDW measurement and SOFA score assessment, which allowed to perform an insightful statistical analysis, according to ‘ordered logistic regression mixed effects model’. Indeed, by using this approach, we revealed a significant direct correlation between MDW and SOFA dynamics (p<0.001). As conceivable, we observed that, in most cases, SOFA score was chiefly determined by the level of respiratory dysfunction; notwithstanding, SOFA score could further increase when additional organ impairments occurred. Interestingly, in those few cases without severe acute respiratory failure, i.e. with good PaO2/FiO2 (>300-400 mmHg, scoring 0-1 points according to SOFA calculation rules for respiratory function), but characterized by higher (>4) total SOFA scores, due to other organ impairments (often related to pre-existing comorbidities), we detected low MDW values, as well as low general inflammation levels. Indeed, in this group (n=16), the correlation between MDW values and the PaO2/FiO2 score alone (calculated according to SOFA rules) resulted to be still significant (p<0.001). These findings may be well in agreement with the primary role proposed for monocyte/macrophage population in the development of inflammatory lung injury, characterizing severe COVID-19 pneumonia [1–3].
Finally, in 21 out of 87 COVID-19 patients, we were able to perform at least 7 serial MDW detections for each case, allowing to uncover interesting patterns of MDW trends and, when possible, to observe notable associations with COVID-19 clinical evolution. In Figure 3, we reported two noteworthy clinical courses with favorable outcome (upper panels), both showing a critical phase, with life-threatening respiratory dysfunction (Pa02/FiO2 <200 mmHg), followed by complete recovery after tocilizumab infusion, performed as immunosuppressive treatment, according to local therapeutic protocols [18]. Both patients obtained a progressive reduction of inflammatory signs and SOFA score. However, IL-6 plasma levels showed massive bursts –up to 1 log, for several days– soon after tocilizumab administration, as result of the IL-6 receptor (IL-6R) competitive inhibition, specifically induced by such monoclonal antibody therapy [21]. This effect can obviously blur the role of IL-6 testing in patients treated with tocilizumab. Besides, MDW patterns well followed the course of the disease, with MDW peak values (>26.4) detected during the utmost critical phase, while, few days after tocilizumab infusion, MDW values progressively decreased till to normal values (<20.5). Of note, at time of discharge, both patients still showed abnormal IL-6 levels, but <20.5 (negative) MDW values. In line with these observations, a recent single-cell analysis in two severe COVID-19 patients showed important monocyte subset modifications after tocilizumab therapy [7]. Functional studies are warranted to explore further the connections between MDW, cytokine levels and cytokine-targeted immunomodulatory treatments.
{kind=link}