The majority of the sample were above 18 years old, with a percentage of 94%, while females constituted 64% of the sample. Regarding the characteristics of the tumor, we found most common side affected by the tumor is the left side of the brain with a percentage of 55% of the participants, while 37% of the patients had a tumor on the right side of the brain. Also, the brain median line (bilateral) had the lowest prevalence among the sample members. As for the location of the tumor, the most prevalent site among the participants was the parasagittal/falx meningioma, with a percentage of 40%, followed by the convexity meningioma, with 30%, and lastly, the sphenoid wing meningioma. About 70% of the patients had headaches, only 44.9% of the patients had cerebral edema, and 47.47% had a neurological deficiency. The greatest proportion of the sample members 56.57% had a meningioma size of more than 4 cm. In addition, 43.4% of the patients had preoperative seizures and this percentage decreased to 25% in post-operative cases. Also, it was found that 43% of the participants had preoperative anti-epileptic treatment, while 96% of the participants had postoperative anti-epileptic treatment. The majority of the sample did not suffer from any comorbidities, while 6% of them had hypertension, 4% had diabetes, 4% had both diabetes and hypertension, and 1% had asthma. 98% of the patients did not undergo radiation previously. Most of the sample who underwent surgical treatment did not develop a tumor after the surgery, with a percentage of 82%. Furthermore, the majority of the participants had grade I (benign) meningioma, as their percentage reached 76%. In contrast, grade II meningioma constituted the second highest prevalence, while grade III had the lowest prevalence. As for postoperative complications, 94% of the patients did not suffer any, while the remaining 6% were distributed between redness, right eye extrusion, right eyelid edema, left conjunctival hemorrhage, complete left eye blindness, left temporal blindness, and renal failure.
Independence tests were done to study the correlation between the occurrence of pre/postoperative seizures and multiple variables, and we found:
-
There is a statistically significant correlation between the classification of meningioma and the occurrence of both preoperative and postoperative seizures (SIG < 0.05). 66.7% and 56.3% of the patients who had grade II meningioma had preoperative and postoperative seizures, respectively. Also, 75% and 50% of patients with grade III meningioma had preoperative and postoperative seizures, respectively.
-
Cerebral edema is statistically associated with preoperative seizures (SIG < 0.05) where 60.5% of meningioma patients had preoperative seizures. In contrast, there was no association between cerebral edema and postoperative seizures (SIG > 0.05) as 67.4% of meningioma patients with cerebral edema did not have postoperative seizures.
-
Neurological insufficiency was statistically not associated with preoperative nor postoperative seizures (SIG > 0.05) as 56.5% and 67.4% of meningioma patients with neurological deficits did not have preoperative and postoperative seizures, respectively.
-
Meningioma size above 4 cm had no correlation with seizures (SIG > 0.05) as 50.9% and 69.1% of patients who had tumor size above 4 cm did not have preoperative and postoperative seizures, respectively.
-
Neither side nor location of the tumor was statistically associated with pre/postoperative seizures (SIG > 0.05).
-
100% of patients below 18 years old had preoperative seizures hence age was statistically associated with preoperative seizures (SIG < 0.05); however, postoperative seizures were not correlated to age (SIG > 0.05).
-
There was no correlation between gender or previous radiation with pre/postoperative seizures.
Moving onto the results of Differences tests for double samples tests, we found a significant difference in terms of the number of seizures occurrence pre and post-operation, as the incidence of seizures has decreased after surgery. Also, it was statistically proven that the usage of antiepileptic drugs was increased postoperatively compared to its usage preoperatively. In addition, to study the effect of risk factors on the occurrence of seizures after and before surgery in patients who underwent surgical resection, binary logistic regression was done, and we found there is a relationship between tumor classification and the occurrence of preoperative seizures (SIG < 0.05). Also, the value of the coefficient of determination according to Cox & Snell R Square was 0.083, meaning that 8.3% of the changes in the dependent variable (preoperative seizures) are made by the independent variable, which is the type of tumor, while according to Nagelkerke R Square, the value of the coefficient of determination was 0.111, where 11.1% of the changes in the dependent variable, the occurrence of seizures, was explained by the independent variable, the grade of tumor. Additionally, it was found that the SIG value of the Who grade variable is less than 0.05 and therefore, there is a significant effect of tumor grade on the occurrence of preoperative seizures. Moreover, grade III of the tumor was also selected as a reference group to compare whether the other groups differed significantly from them in terms of the incidence of seizures, and we found that SIG value of the first group (grade I) of the independent variable is less than 0.05 and therefore, there is a statistically significant difference between the first and third grade of tumor in terms of the incidence of seizures. The Exp(B) value was 0.184 less than one, and therefore when the patient has grade I meningioma, the probability of the event (preoperative seizure) is less than the probability of a preoperative seizure in those with a grade III meningioma. In contrast, it was found that SIG value of the second group (grade II) of the independent variable is greater than 0.05 and therefore there is no significant difference between the second grade of tumor and the third grade of the tumor in terms of the incidence of seizures. The Exp(B) value was 0.667 less than one, and therefore when the patient has a grade II meningioma, the probability of the event (preoperative seizure) is less than the probability of a preoperative seizure in those with a grade III meningioma. In addition, we found there is a correlation between tumor classification and the occurrence of postoperative seizures (SIG < 0.05). Moreover, the value of the coefficient of determination according to Cox & Snell R Square was 0.122, meaning that 12.2% of the changes in the dependent variable (postoperative seizure) are made by the independent variable, which is the type of tumor. While according to Nagelkerke R Square, the value of the coefficient of determination was 0.181, meaning that 18.1% of the changes in the dependent variable are made by the independent variable, the tumor type. It was found that SIG value of the Who grade variable is less than 0.05 and therefore there is a significant effect of tumor grade on the incidence of postoperative seizures. Grade III of the tumor was also selected as a reference group to compare whether the other groups differed significantly from them in terms of the incidence of seizure. We found that SIG value of the first group of the independent variable is less than 0.05 and therefore there is a significant and statistically significant difference between the first and third grade of tumor in terms of the occurrence of postoperative seizure. The Exp(B) value was 0.19 less than one and therefore when the patient has a grade I meningioma, the probability of the event (postoperative seizure) is less than the probability of having a postoperative seizure of a grade III meningioma patient. Also, SIG value of the second group of the independent variable is greater than 0.05 and therefore there is no significant difference between the second grade of tumor and the third grade of the tumor in terms of the incidence of seizure. The Exp(B) value was 0.775 less than one, and therefore when the patient has a grade II meningioma, the probability of the event (postoperative seizure) is less than the probability of postoperative seizure in a patient with a grade III meningioma.
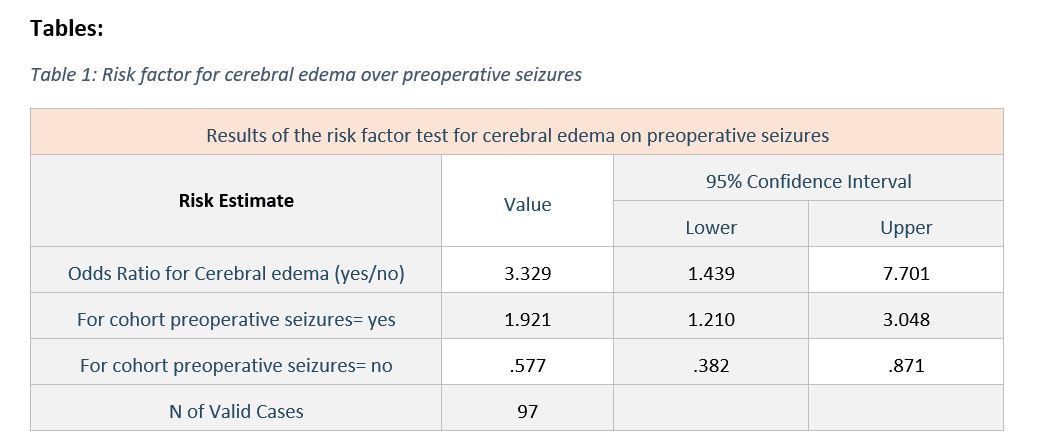
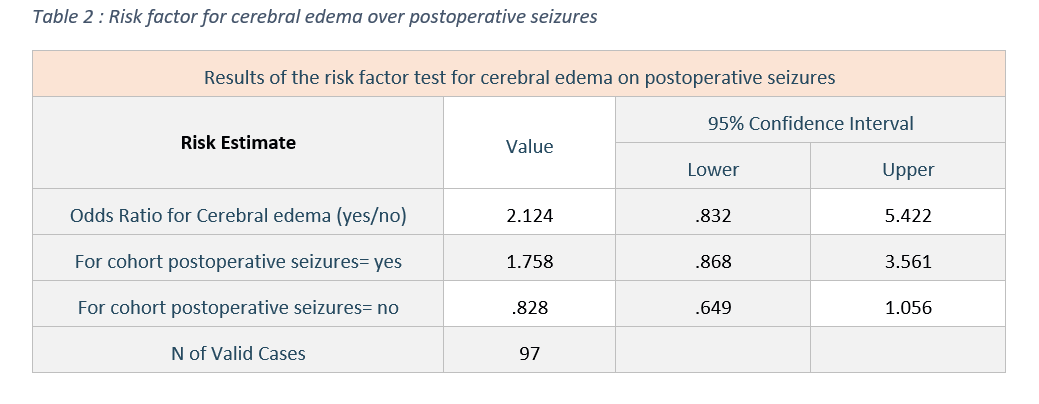
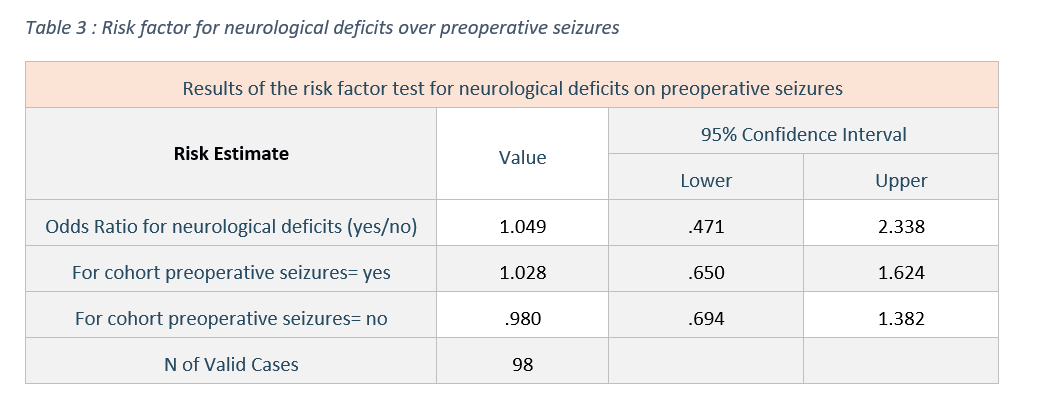
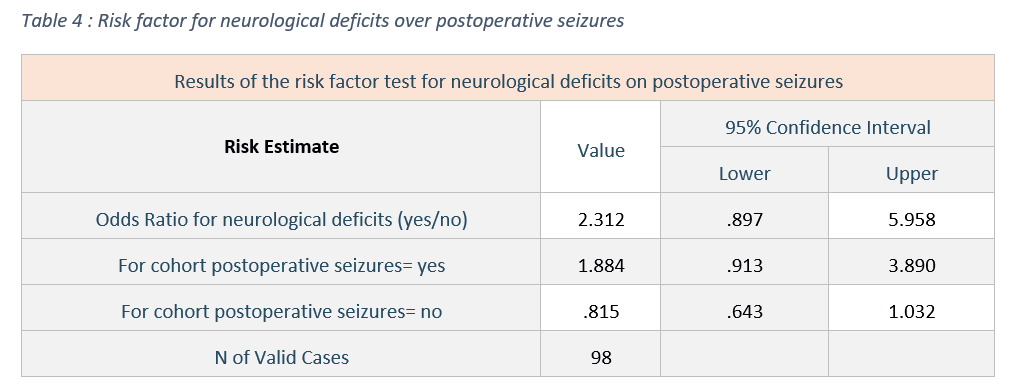
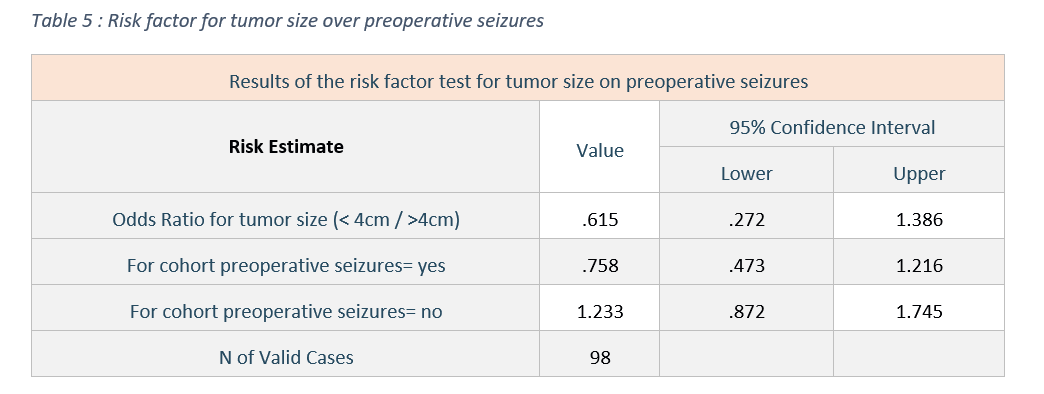
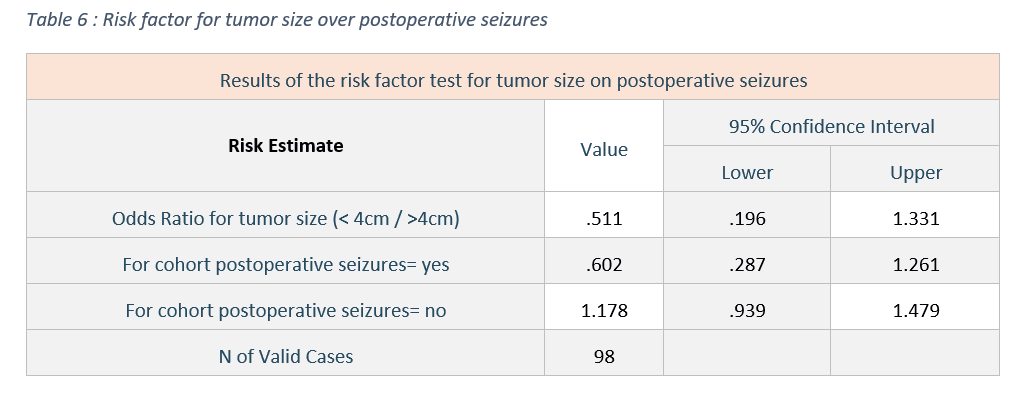
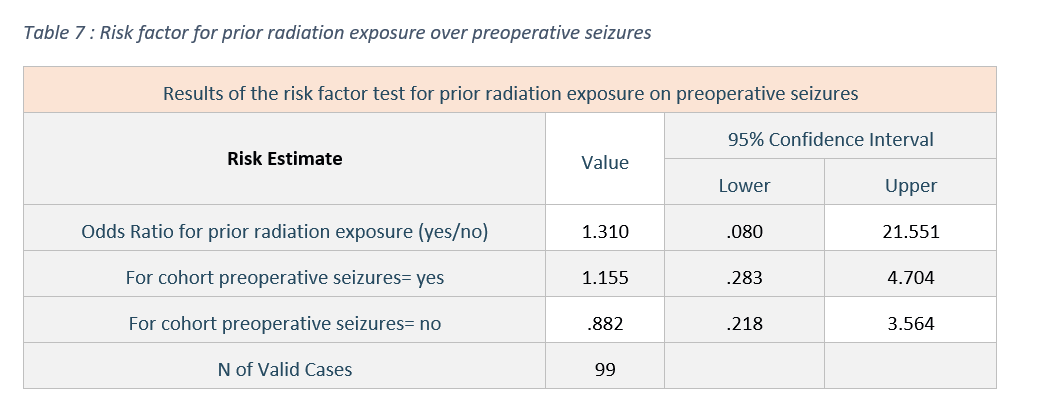
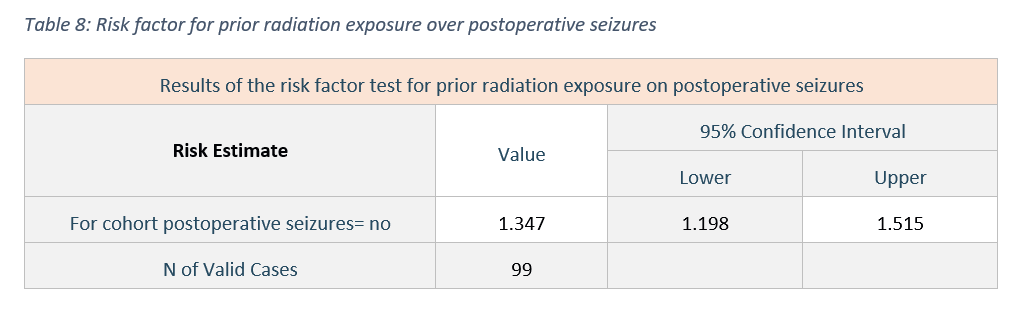
Furthermore, the relative risk test was used to determine the degree to which the studied event will occur in the presence of the risk factor. Firstly, we found that if the meningioma patient has cerebral edema, the probability of having a preoperative seizure is 2.32 higher than the probability of not having a seizure, and the incidence of preoperative seizures for people with cerebral edema was 0.92 higher than the incidence of preoperative seizures for people without cerebral edema Table 1. Meanwhile, if the meningioma patient has cerebral edema, the probability of having a postoperative seizure was 1.124 higher than the probability of not having it, and the incidence of postoperative seizures for people with cerebral edema was 0.758 higher than the incidence of postoperative seizures for people without cerebral edema Table 2. As for the neurological deficiency, if it was present in meningioma patients, the probability of having a preoperative seizure was 0.049 higher than the probability of not having a preoperative seizure, and the incidence of preoperative seizures for patients with neurological deficits was 0.02 higher than the incidence of seizures for patients without neurological deficits Table 3. Meanwhile, the probability of having a postoperative seizure for individuals with a neurological deficiency is 1.312 higher than the probability of not having a postoperative seizure, and the incidence of seizure for individuals with neurological deficiency is 0.02 higher than its incidence for individuals with neurological deficits Table 4. As for the size of tumor, it was found that if it’s less than 4 cm, the probability of preoperative seizures occurrence is 0.385 less than the probability of not occurring, and the rate of not having a seizure with tumor size less than 4 cm is 0.23 higher than the rate of not having a seizure for individuals with a tumor size more than 4 cm Table 5. Meanwhile, the incidence of postoperative seizures for patients with tumor size less than 4 cm is 0.489 less than the incidence of not having postoperative seizures, and the incidence of not having a seizure for patients with tumor size less than 4 cm was 0.17 higher than incidence of not having a seizure for tumor size more than 4 cm Table 6. In addition, patients who have been exposed to prior radiation had a 0.31 higher probability for having preoperative seizure than the probability of not having it, and the probability of having preoperative seizures for individuals who have been exposed to radiation previously was 0.155 higher than the probability of not having it for patients who have not been exposed to radiation Table 7. Meanwhile, no value was given for the probability of postoperative seizures in individuals who had prior radiation exposure, and the rate of not having a postoperative seizure for patients exposed to prior radiation was 0.347 higher than the rate of not having it in patients who have not been exposed to prior radiation Table 8.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}