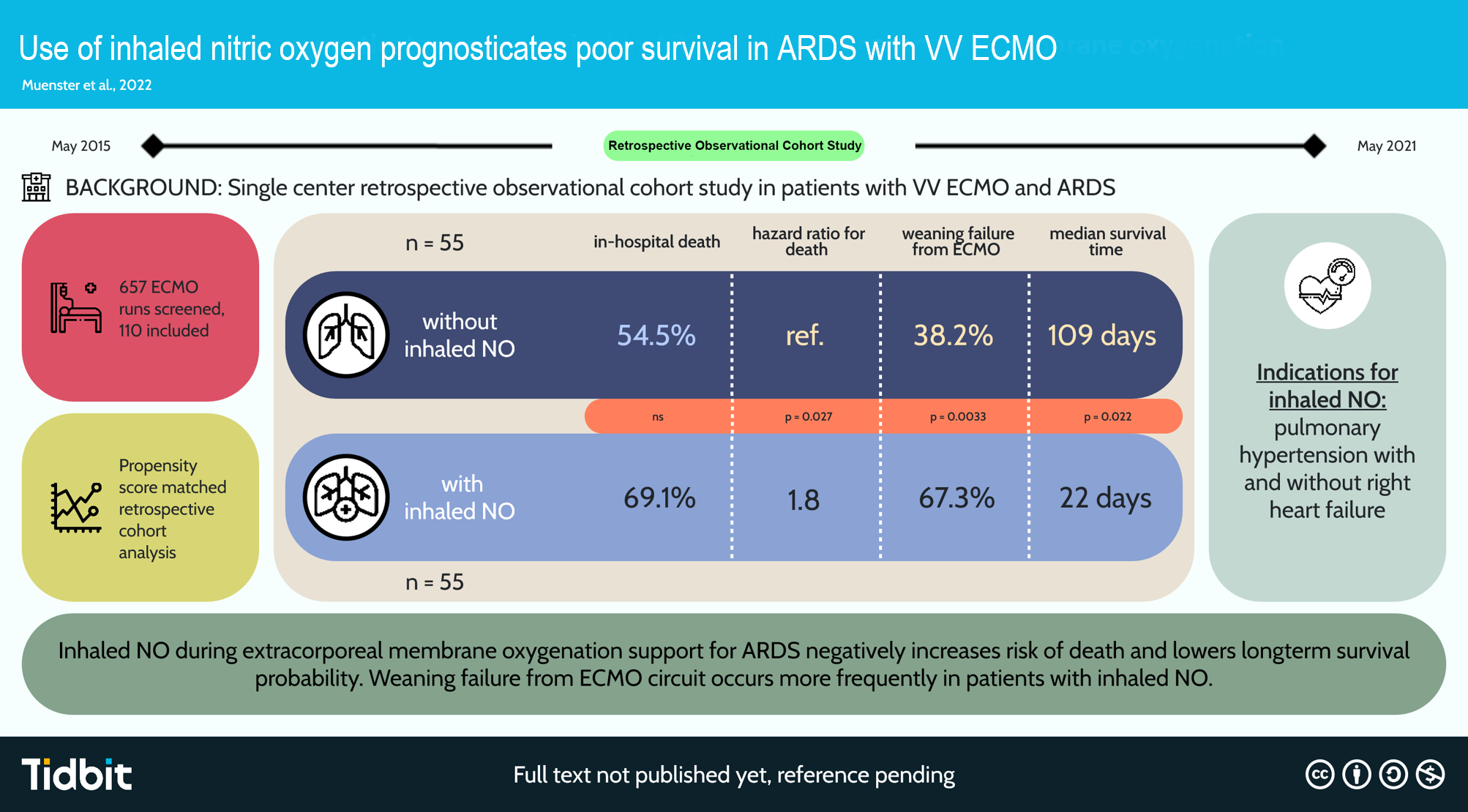
The main finding of this propensity-matched cohort study is reduced survival probability and an increased hazard ratio for in-hospital mortality despite iNO administration in patients with severe ARDS under VV ECMO.
Pulmonary vascular dysfunction is one of the pathophysiological hallmarks of ARDS and ultimately leads to a certain degree of PAH (36). Recent data suggest that PAH and subsequent RV failure are medical burdens that occur in every second patient with moderate to severe ARDS and are independently associated with the risk of mortality (36, 37). In ARDS, multiple pathophysiological mechanisms that directly cause injury to pulmonary circulation include endothelial dysfunction, distal pulmonary vascular occlusion at the capillary level, pulmonary vasoconstriction, extrinsic vessel occlusion by alveoli distention, and, ultimately, vascular remodeling (38). These mechanisms lead to increased pulmonary vascular resistance, precapillary pulmonary hypertension, and increased RV afterload (38). The uncoupling between pulmonary circulation and the right heart ultimately leads to the breakdown of oxygen delivery.
Various strategies, including limiting volume loading and correcting blood pressure by infusing norepinephrine, have been suggested to decrease RV wall stress and RV end-diastolic pressure, thereby improving RV stroke volume (39). The patients of the current study received a restrictive fluid regimen and norepinephrine to avoid hypotension, as described previously (35).
Both hypoxia and hypercapnia strongly increase pulmonary vasoconstriction and contribute to PAH (40). Severe ARDS per se is associated with profound hypoxia, which may be accompanied by hypercapnia (41). Hypercapnia is the consequence of protective ventilatory strategies designed to reduce ventilator-induced lung injury. It also reflects increased dead space due to alveolar overdistension and ARDS severity (42).
Higher PEEP levels are frequently required in severe ARDS to avoid life-threatening hypoxia. However, transpulmonary pressure, despite low tidal ventilation when lung compliance decreases due to alveolar collapse, may be associated with increased end-inspiratory airway pressure (43). Consequently, pulmonary capillaries become stretched and their caliber is reduced, resulting in increased pulmonary vasoconstriction (44, 45).
By controlling arterial oxygenation and decarboxylation, even during ultraprotective ventilation (41), VV ECMO suppresses the major factors that increase pulmonary vascular resistance and cause PAH in severe ARDS, thereby sufficiently unloading the RV (46). In this study cohort, VV ECMO was indicated to correct hypoxemia and hypercapnia, as well as allow ultraprotective ventilation, to prevent peak inspiratory (> 27 cmH2O) and/or driving (> 15 cmH2O) pressure (Table 3). Although VV ECMO initiation in the current study resulted in adequate arterial oxygenation and normocapnia at a peak inspiratory and driving pressures < 25 cmH2O and < 10 cmH2O, respectively, PAH with or without RV failure persisted in 23% of the patients with severe ARDS.
Although iNO in ARDS has been widely abandoned by intensivists because RCTs and meta-analyses have demonstrated no benefits for survival despite temporal improvement in oxygenation (18, 19), it may be an option for decreasing RV afterload by lowering PAH (36). Intriguingly, however, this specific cohort presented with significantly reduced survival probability and an increased hazard ratio for in-hospital mortality with iNO administration.
These findings raise the question of whether iNO itself or the persisting PAH or RV failure may be the contributing factor. iNO use in ARDS has been widely studied over the last decades, and no evidence of direct NO toxicity has been observed at clinically relevant doses below 20 ppm (47). However, conflicting evidence has been reported on whether iNO contributes to increased acute kidney injury (48, 49). CKRT in this study did not indicate an increased rate of acute kidney injury before or during VV ECMO (Table 2). Thus, the potentially detrimental effects of iNO on kidney function can be excluded as a cause of increased mortality.
The optimal dose and time of iNO treatment in ARDS remains controversial. A European expert recommendation on the use of iNO in adults with ARDS suggested that toxic side effects (e.g., methemoglobinemia and the formation of relevant nitrogen dioxide levels) are less likely when inhaled NO doses stay < 20 ppm (47). Initiating iNO treatment as early as 24–72 h after the onset of ARDS has been suggested because iNO is mainly effective during the early onset of ARDS. In this study, an average iNO dose of 14.5 ppm was administered, and iNO delivery was performed for a median duration of 3 days. iNO was initiated within 24 h after the diagnosis of either PAH and/or RV failure. In most of the patients, iNO was initiated during VV ECMO, as opposed to before or after VV ECMO, as administered in a small cohort. The current analyses revealed an increased hazard ratio for in-hospital mortality when iNO was used during VV ECMO support. In contrast, iNO administration before or after VV ECMO did not significantly affect the hazard ratio for in-hospital mortality. However, the number of included patients in both subgroups was too small to draw relevant conclusions in terms of in-hospital mortality. Intriguingly, a positive response to iNO was observed in only 30% of the patients of the current study. Similar findings were reported by Manktelow (50) on severe ARDS with septic shock. These studies were conducted before the widespread availability of VV ECMO and ultraprotective ventilator strategy. The data of the current study confirms the validity of this observation despite the use of current protective treatment regimens.
Other cofactors that may have contributed to the reduced survival probability and increased risk in the study cohort, i.e., age, sex, and disease severity at the time of VV ECMO initiation (indicated by SOFA score), were adjusted through propensity score matching. However, the iNO itself neither can be proven to reduce survival nor increase the risk of mortality due to the retrospective nature of the data collection.
Overall, the indication for iNO in this specific patient cohort (severe ARDS and VV ECMO) can be concluded to be a negative predictive variable for survival and risk of mortality. This cohort suffers from multiple comorbidities, all of which will worsen the clinical course of the patient regardless of iNO administration. Of note, the current study demonstrated that both groups did not differ in terms of comorbidities as indicated by the Charlson Comorbidity Index. This is further supported by the implementation of iNO in these patients as rescue therapy. The RCT conducted in the late 1990s that first described the use of iNO was performed in patients with mild to moderate ARDS. Thus, iNO administration in critically ill patients with severe ARDS under VV ECMO support should be very carefully discussed because beneficial effects are more than questionable in this specific patient cohort.
A limitation of this study is the retrospective and monocentric nature of the analyses. The availability of RCTs involving patients with severe ARDS is limited after initial RCTs failed to demonstrate any beneficial effects of iNO on survival and mortality. To further improve the significance of the current analyses, a propensity-matched approach in a large cohort of 479 patients under ECMO support was selected. The use of SOFA as a severity of illness matching estimate may not capture the true severity of illness in each group. However, none of the established ECMO outcome prediction scores is able to represent an additional treatment option (such as iNO) during ECMO support. The RESP-Score did not differ between groups. Nevertheless, retrospective analyses allow for an unbiased selection process of patients. All included patients were analyzed depending on treatment and thus were not subjected to selection bias for iNO treatment.
The possibility that RV failure per se contributed to the reduced survival probability cannot be excluded because the iNO treatment itself can only be analyzed. Intriguingly, no signs of PAH or RV failure were found in the propensity-matched cohort without iNO. Hence, iNO use indicates reduced survival probability but most likely does not cause it.
In summary, iNO administration in patients with severe ARDS and concomitant VV ECMO support was demonstrated to be a negative predictive variable of survival probability and risk of mortality. iNO in this specific cohort was concluded to only be recommended as a rescue therapy with questionable outcomes when all other options fail.
{kind=link}