The magnitude of unfavourable management outcome of IO at Chiro General Hospital was
21.3%. The most unfavourable management outcome of IO was wound site Infection. In
current study Old age, late presentation of illness and pre-operative diagnosis of
gangrenous bowel were significantly associated with the occurrence of unfavorable
management outcome of Intestinal Obstruction.
This is in line with the study done Adama(24.6%)[
10
</a>] and India (25.89%)[<a href="#_ENREF_11">
11
</a>]. But the magnitude of unfavourable management outcome of IO in this study was low
compared with the reported studies done at Canada (64%)[<a href="#_ENREF_12">
12
</a>] and Nigeria(66.5%)[<a href="#_ENREF_13">
13
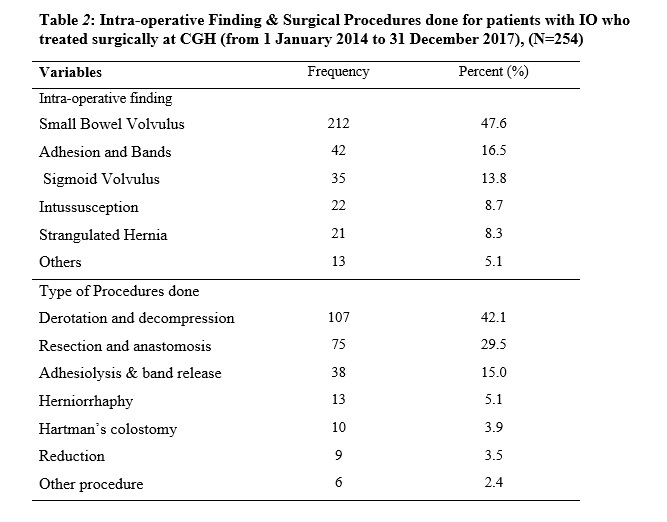
</a>] . This difference may be the cause of IO and type of procedure done (intussusception
was the most cause of IO by which highest R&A was done while R&A was significantly
associated with management outcome) a study done at Nigeria. This difference may be
different studying population and different mean age a study done in both studies.
On the contrary, this magnitude was higher than the study done in Kenya (13.6%)[<a href="#_ENREF_14">
14
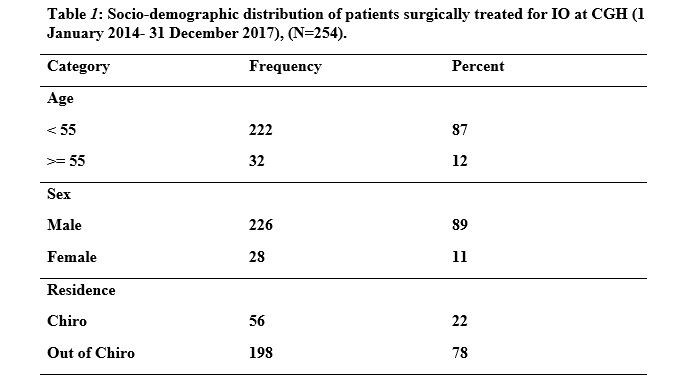
</a>]. The possible difference may be residence of a patient in which there were lower
proportion of patient came from rural dweller (58.7%)[<a href="#_ENREF_14">
14
</a>] than this study (78%). Patient who came from urban area or area near to hospital
have good awareness on the importance of getting health service early, hence early
intervention had lower unfavourable outcome. The other possible reason for the difference
SOP (Standard of Procedure) may be applied more properly in the study area of Kenya.
Following SOP for every procedure decrease the acquisition of microorganism into surgical
wound, hence the lower the infectious organism, the lower the magnitude of unfavourable
outcome. </p>
The most post-operative complication was wound site infection (hematoma& incisional
SSI) 30(55.5%) followed by post-operative pneumonia 08(14.8%), Anastomotic leak 06(11.1%),
05(9.3%) respectively. The most post-operative complication was similar a study done
at Adama, Kenya and Nigeria which accounts 39.3%, 33% and 31.4% respectively among
patient develop complication [
10
</a>, <a href="#_ENREF_13">
13
</a>, <a href="#_ENREF_14">
14
</a>]. But a study done at Canada the most post-operative complication was respiratory
complication like pneumonia [<a href="#_ENREF_12">
12
</a>] which is second complication in this study. This difference may be the lower proportion
of malnutrition patient & poor health-seeking behavior and higher standard of life
modification style including hygiene in developed nation such as Canada than developing
nation such as Ethiopia and other African countries.</p>
Unfavorable outcome of patients with IO was affected by the cause of obstruction,
duration of illness, age and complication detection time. [
15].
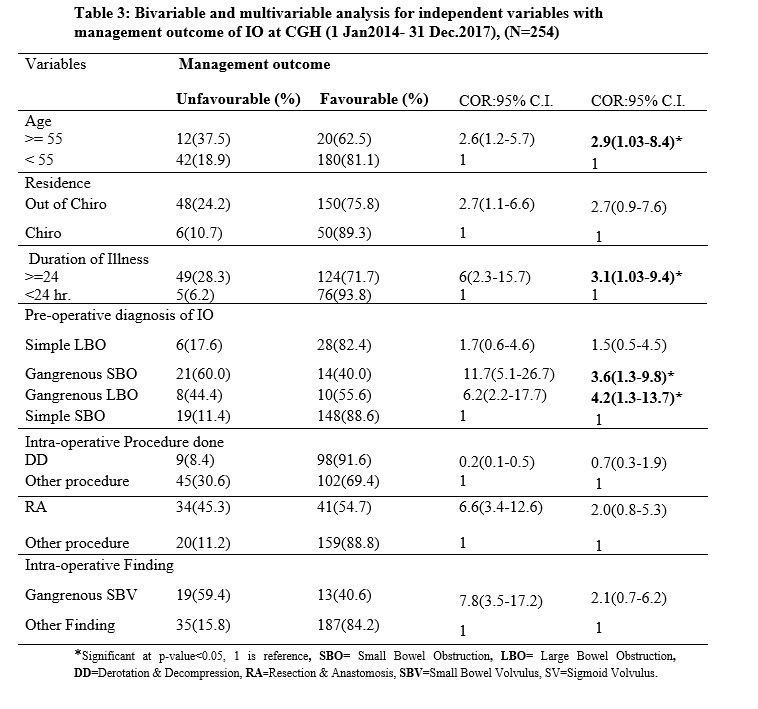
In this study, being old age (age ≥55 years) was nearly 3 times more likely to develop
unfavorable management outcome of IO, compared with those patients whose ages less
than 55 years. This was in line with a study done Gondar [
5]. This study was contradict with a study done in Adama [
10
</a>],in which age of patients were not significant predictor of unfavourable outcome.
This may be due to old age group in study area may came early, hence high proportion
of favourable outcome. </p>
Generally outcome of patient with surgically treated for IO might be affected by
different factors, such as age of patient, residence of patient, duration of illness,
cause of obstruction, viability of bowel, type of procedure done and length of hospital
stays.
Duration of illness before surgical intervention has significant statistical association
with unfavorable management outcome of patients with IO. Patient who came late were
about three times more likely to develop unfavorable management outcome, compared
patients who came early. This study was similar a studies done in Adama [
10
</a>] and Gondar [<a href="#_ENREF_5">
5</a>], in which patients who came late had higher propotion of poor outcome. This was
possibly due to poor health-seeking behavior and poor transportation system in this
sub-region. Late presentation in case of intestinal obstruction accounts for disastrous
outcomes, notably high rate of complications, long hospital stay and high mortality
rates[<a href="#_ENREF_2">
2</a>].</p>
In this study unfavorable management outcome of patient with IO were significantly
affected by intra-operative finding of gangrenous bowel. Patients with gangrenous
SBO and gangrenous LBO were more likely to develop unfavorable management outcome
of patient with IO, compared with patients with simple SBO. This study was in line
with a study done at Adama [
10
</a>].</p>
In this study gender of the patients did not influence the outcome of treatment in
terms of morbidity and mortality. This also same in study done at Adama, Nigeria,
Ruanda [
10,
13,
16].
In this study unfavorable management outcome were not significantly affected by Intra-operative
procedures of bowel resection and anastomosis. This was in contrary with a studies
done at Nigeria, Kenya and Adama [
10
</a>, <a href="#_ENREF_13">
13
</a>],in which RA were significantly increase the outcome of unfavourable management outcome.
</p>
In this study since it was a document review ,some data’s were incomplete, as well
poor hand writing in some cards and even few cards were missed.
It was impossible to measure some essential parameters, which may significantly contribute
for Unfavorable outcome of IO like Educational status of the patients, Occupational
status, and House hold income per month since, secondary data was utilized in this
study.
There was scarcity of data available in the country, and no similar published data
from the region which makes difficult in comparisons of the study.
The results of the study may not show the actual picture of the problem in the community
since this study was a facility based study.
{kind=link}
{kind=link}
{kind=link}