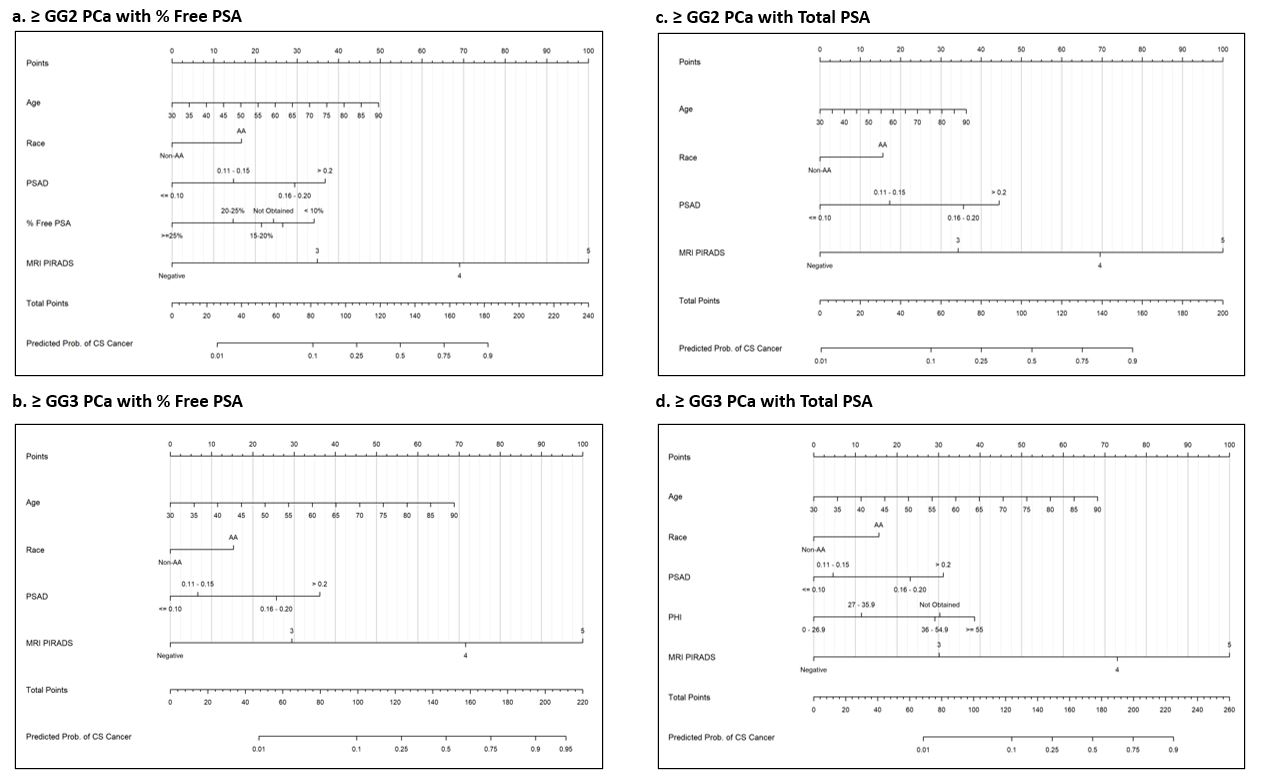
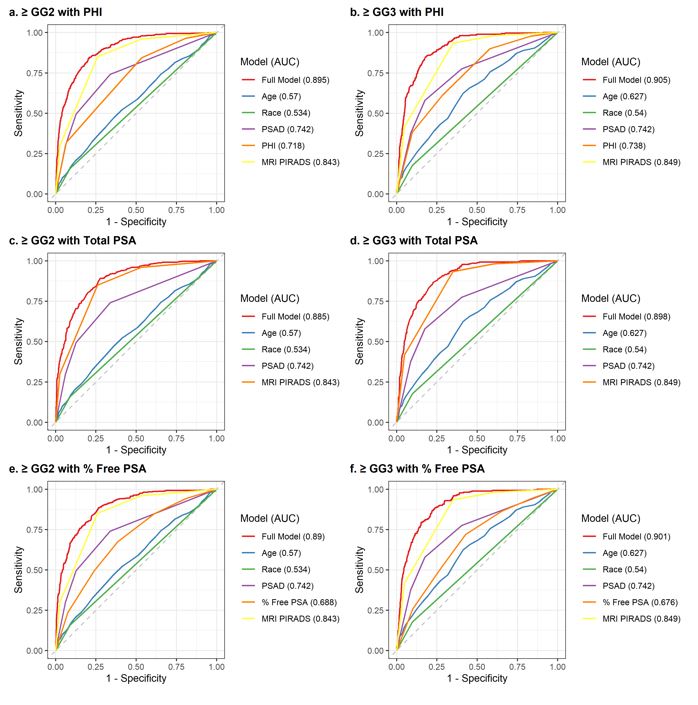
We used real-world data from our large academic system incorporating serum biomarker data (PHI, % free PSA or total PSA) and mpMRI along with other clinical variables to develop nomograms that can improve detection of csPCa and higher grade PCa while significantly reducing unnecessary biopsies. We created adaptable versions of the nomogram based on available serum biomarkers and openly published the tool for transparent and wider adoption. Performance of the models was high with accuracies of ≥ 0.885 in the training cohort and ≥ 0.896 in the independent validation cohort.
Traditionally, PSA based screening has been marred by overdiagnosis and overtreatment. Originally, studies evaluated patient factors like age, race, and PSAD for risk stratification. Advanced serum- and urine-based markers such as 4k score, MyProstateScore, and SelectMDx have also been developed to further enhance the detection of csPCa.(13) While these markers offer clinical value when used individually, biopsies avoided are based on a prior paradigm of detection by TRUS biopsy with uncertain utility in conjunction with mpMRI. For example, setting the PHI threshold at 28.6 avoids 30% of TRUS biopsies.(14) Similarly, 4kscore cut-off of 20% risk of cancer reduces the number of biopsies by 36% while delaying diagnosis of csPCa in 4.7%, but performance in a mpMRI-based diagnostic approach is unknown.(15) Moreover, these tools are not able to localize csPCa within the prostate at the time of biopsy if one is performed.
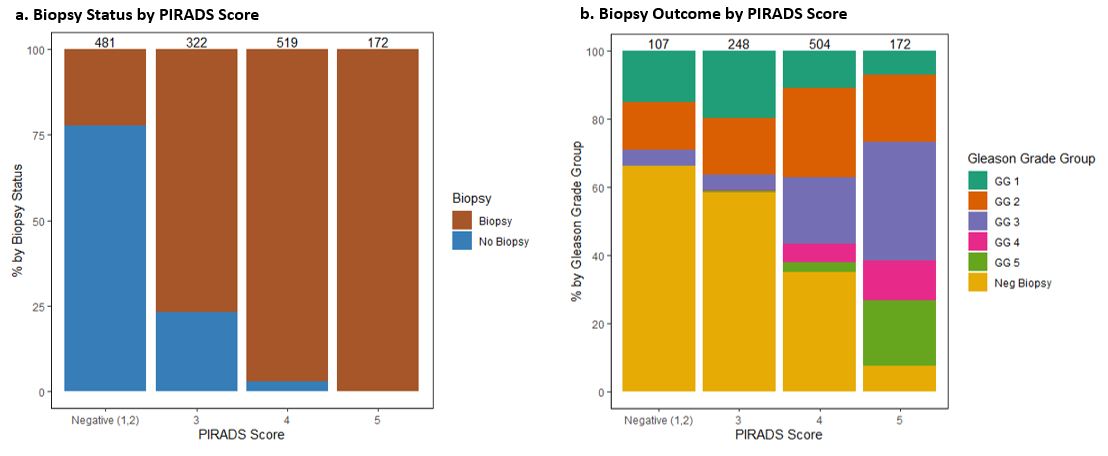
Therefore, there is a strong interest in combining advanced serum biomarkers with mpMRI, as the advent of mpMRI has greatly improved our ability to detect csPCa. In the PRECISION trial, mpMRI avoided 28% of primary biopsy while diagnosing 13% fewer clinically insignificant cancers.(16) Furthermore, targeting mpMRI lesions increased detection of csPCa by 12% compared to standard TRUS biopsy. However, the sensitivity and specificity of mpMRI for csPCa vary across studies, ranging between 58–96% and 23–87% respectively.(17) This variability is significant for commonly biopsied PIRADS 3 and 4 lesions, which is also reflected in our experience (Supplemental Fig. 1) with 83% and 46% of PIRADS 3 and 4, respectively, having clinically insignificant (Negative or GG1) outcome. By combining MRI with other biomarkers and clinical variables, we believe that unnecessary biopsies, particularly among men with PIRADS 3 lesions mpMRI, can be largely avoided.
Nomograms offer an avenue to combine various advanced screening tools to improve patient risk stratification, and have been shown to offer higher accuracy for predicting outcomes in comparison to other predictive tools, such as look-up tables or decision trees.(18–20) In fact, a national survey of radiation oncologists and urologists found that 60% of providers were familiar with prostate cancer nomograms, 55% used nomograms routinely in their practice, and 74% found nomograms to be user friendly.(21) Nomograms in urology were pioneered by Kattan and colleagues predicting likelihood of disease recurrence and progression. Since then, various validated nomograms have been created at different stages of the prostate cancer disease stages e.g. UCSF-CAPRA score for post-biopsy risk stratification and MSKCC nomograms for pre- and post- radical prostatectomy or for salvage radiation.
Currently, there is no singular widely adopted and validated nomogram that combines advanced screening biomarkers and mpMRI in a pre-biopsy setting to predict risk of csPCa and higher risk PCa. In a recent randomized control clinical trial of STHLM3, combining the Stockholm 3 test with mpMRI reported AUC of 0.76 for their nomogram for csPCa.(22, 23) A retrospective series by Wagasker et al proposed a nomogram combining 4kscore with mpMRI that had AUCs of 0.84 for any prostate cancer, 0.88 for csPCa, and 0.86 for ≥ GG3 prostate cancer.(24) The PROMOD study combined PSAD with mpMRI and evaluated its performance in detection of csPCa in a large retrospective multi-institutional cohort, reporting a high sensitivity of 96.7% but low specificity of 30.1% in their biopsy naïve population.(25) Lastly, as an example of models based on PSA and mpMRI parameters, Kinniard et al developed a nomogram with sensitivity of 90% and specificity of 54% at a biopsy threshold of 20% probability of csPCa, with AUC values of 0.843 and 0.888 in discovery and validation cohorts.
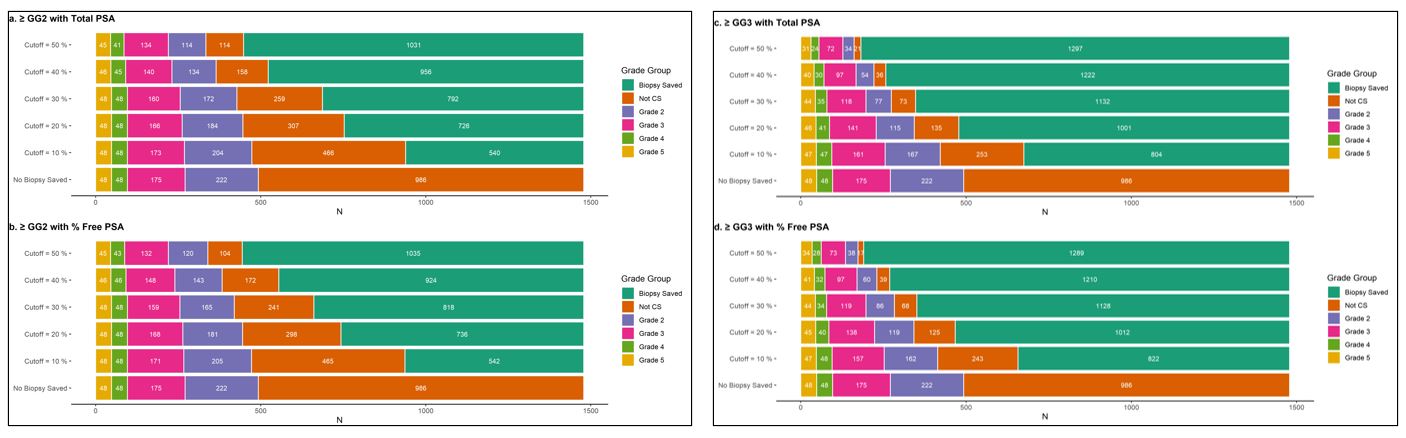
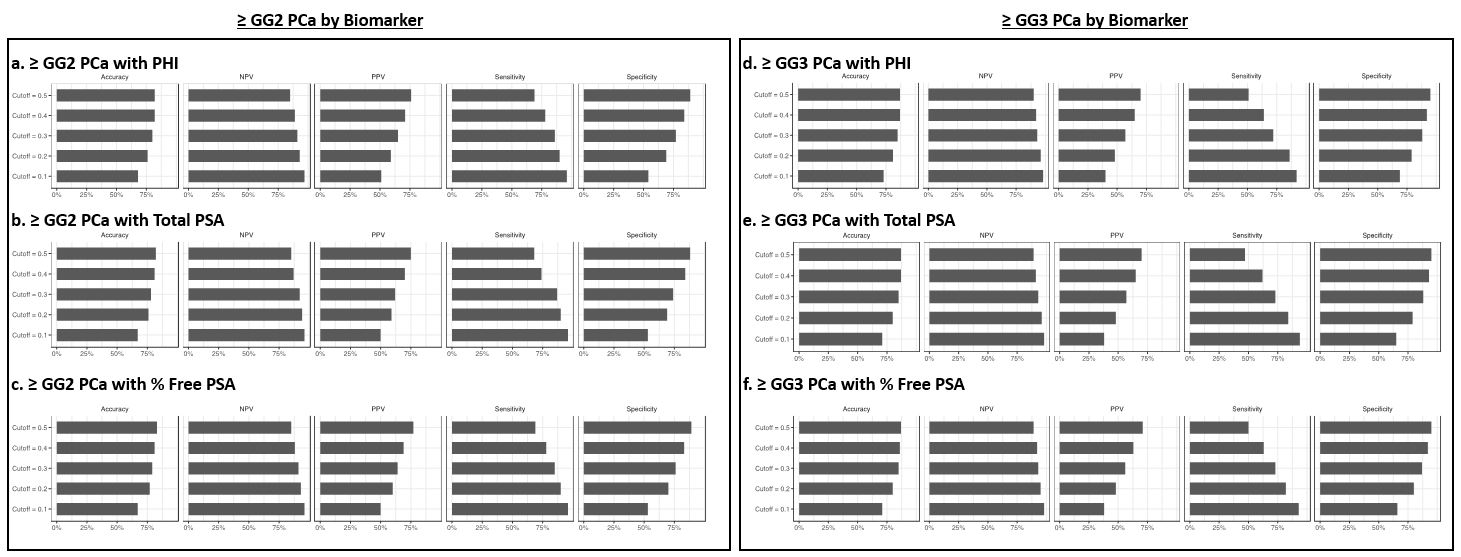
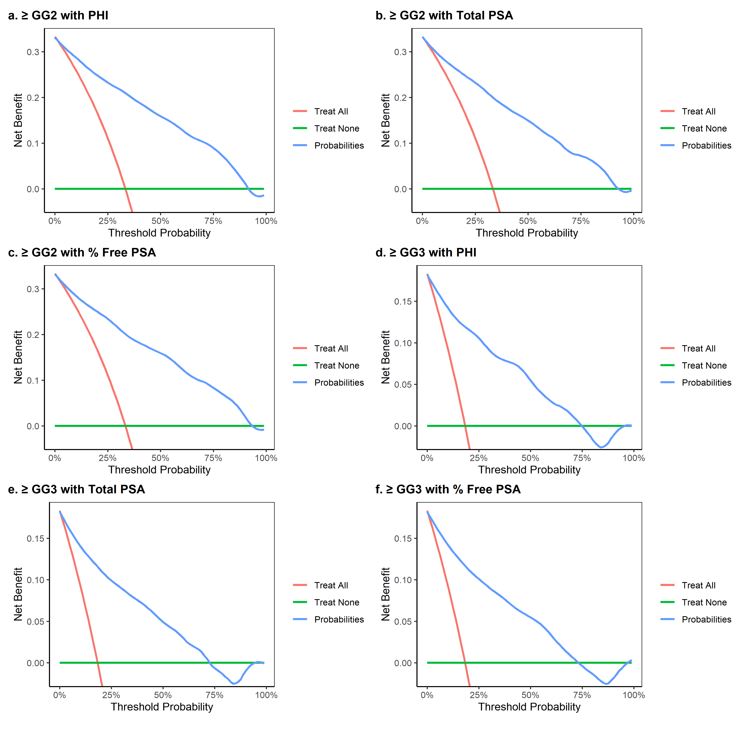
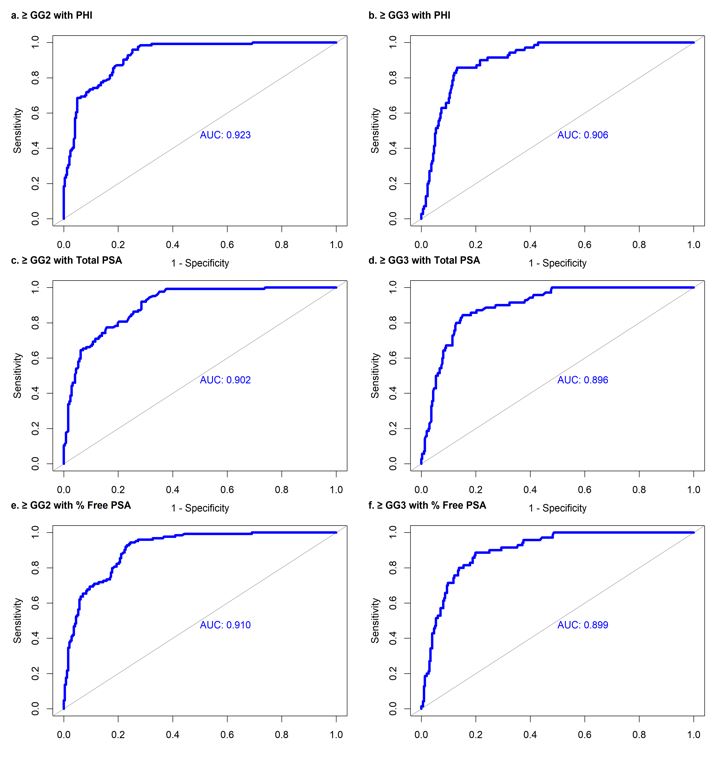
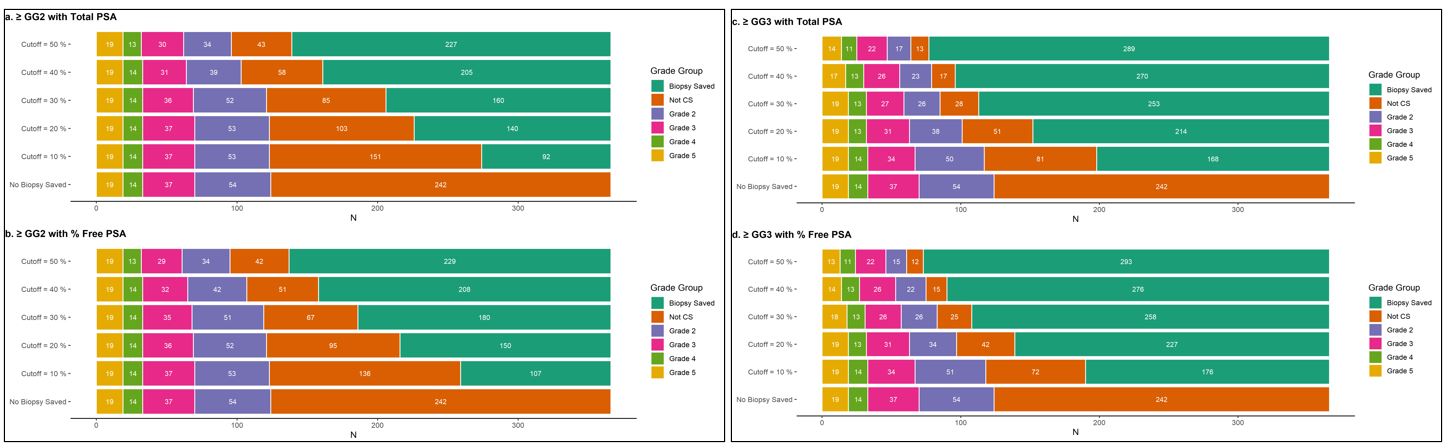
In our cohort, we report a similar high sensitivity of 90%, but with higher specificity of 69% for our model utilizing PHI for prediction of ≥ GG2 prostate cancer. Furthermore, the AUCs for our nomograms are generally superior to those published in the literature, with ≥ 0.885 in the development cohort and ≥ 0.896 in the independent validation cohort. While PHI does make our model more robust, the nomograms utilizing % free PSA and total PSA overall have high discriminatory characteristics in both the development and independent validation cohort, demonstrating the overall versatility of our nomograms across practice settings and preferences. This is best demonstrated in our independent validation cohort, where application of our csPCa model with PHI and biopsy threshold of 20% saved biopsy for 143/366 (39.1%) men while only missing 1 case (0.8%) of csPCa. In comparison, the nomogram for prediction of csPCa with total PSA at a biopsy threshold of 20% similarly saved biopsy for 140/366 (38.3%) men while again only missing 1 case (0.8%) of csPCa.
Furthermore, prior nomograms include both biopsy naïve and prior negative biopsy patients, whereas our nomogram focused on biopsy naïve patients. The rate of csPCa is higher in the biopsy naïve setting compared to prior negative biopsy patients, with the latter inflating estimates of overall biopsies avoided in prior analyses; for example, the PLUM cohort showed 45.8% of biopsies could be avoided among prior negative patients but only 18.1% for biopsy naïve patients.(11, 12) Overall, our nomograms predict csPCa and higher grade PCa with high accuracy and greater potential for avoiding biopsies among biopsy naïve patients.
A few limitations of the present study deserve to be noted. First, it is a retrospective series, which may create a selection bias and not perfectly represent the general screening population. However, we included all men evaluated with serum biomarkers and mpMRI to improve generalizability of our cohort compared to prior analyses where many patients with low suspicion on mpMRI have often been excluded or not captured. Our nomograms assume that men with PIRADS 1–3 not undergoing biopsy would have had a clinically insignificant outcome, potentially inflating nomogram’s performance (specificity, negative predictive value). However, upon review of patients who did not undergo initial biopsy, only 2% of these patients with follow up were found to have csPCa over the median follow-up of 1.8 years, with the majority of these patients having a repeat mpMRI prior to biopsy showing upgrading of highest PIRADS lesions. Therefore, the impact of this assumption is negligible given the low rate of on follow up, demonstrating that men can be safely monitored with serial serum biomarker screening and for cause mpMRI. While we did perform validation with an independent cohort at our institution, further external validation is required across institutions and community practice to establish generalizability of the nomograms. Furthermore, our academic institution has dedicated genitourinary radiologists and pathologists, but application in the community may also be affected by interrater variability among radiologists and pathologists.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}