The present study sought to mitigate IRI in a pig model of hemorrhagic shock and profound ischemia by using a peptide developed to protect mitochondrial function. We observed pleiotropic effects of Elamipretide. Namely, Elamipretide not only reduced the volume of isotonic crystalloids required to maintain normotension, but it also significantly reduced histologic and biochemical evidence of myocardial and renal injury.
We sought to evaluate mitochondrial rescue after severe hemorrhage. Elamipretide is a small peptide developed to augment mitochondrial function for patients with mitochondrial diseases [36]. The drug stabilizes the mitochondrial inner membrane by binding cardiolipin, [29] an abundant mitochondrial membrane phospholipid that exists in microdomains (i.e., distinct membrane regions enriched in cardiolipin). The binding of Elamipretide to cardiolipin preserves mitochondrial cristae structure, improving energy production and reducing the production of damaging mitochondrial reactive oxygen species [29]. Several preclinical research models have shown that this peptide preserves mitochondrial function and provides cytoprotection. For instance, in vivo rabbit [32] and sheep, as well as ex vivo guinea pig [37] myocardial infarction studies, demonstrated a reduction in infarct size with Elamipretide treatment. Similarly, mice with ischemic strokes displayed reduced infarct size and improved neurological function following Elamipretide treatment [38]. In addition, studies in pigs have focused on establishing the benefits of Elamipretide in models of metabolic syndrome [39, 40] and atherosclerotic renal artery stenosis [41]. Most importantly, from a rapid translation standpoint, Elamipretide has already been tested in clinical trials for non-trauma indications, including an atherosclerotic renal stenosis Phase II trial [42], an intermediate age-related macular degeneration Phase I trial [43], and a Phase II-III trial for Barth syndrome, a genetic disorder of mitochondrial cardiolipin metabolism [44]. Yet, the mitochondrial protective effects of Elamipretide have not been thoroughly studied in the context of IRI, even though mitochondrial injury is an essential component of the pathophysiology, as seen in preclinical trauma models. For example, a study utilizing a porcine polytrauma model (hemorrhagic shock with liver laceration, pulmonary contusions, and tibial fracture) demonstrated hepatic mitochondrial injury by electron microscopy and was associated with mitochondrial autophagy, cell apoptosis, and recruitment of anti-inflammatory leukocytes to the liver [45].
Patients in extremis who received lifesaving maneuvers like REBOA will suffer a more severe mitochondrial dysfunction when compared to more traditional resuscitation practices for hemorrhagic shock. The exacerbated IRI is driven by complete or partial aortic occlusion, which likely worsens mitochondrial injury. This could explain the profound vasodilation and distributive shock state often observed in those patients, even after their circulating blood volume is restored with transfusion and volume resuscitation. In addition, this severe IRI drives the need for large ongoing resuscitation requirements and significant vasopressor support, both increasing complications such as acute kidney and lung injury [46]. Therefore, pharmacological interventions that reduce mitochondrial dysfunction in trauma patients with severe IRI may improve morbidity and mortality by influencing the patient's response to resuscitation.
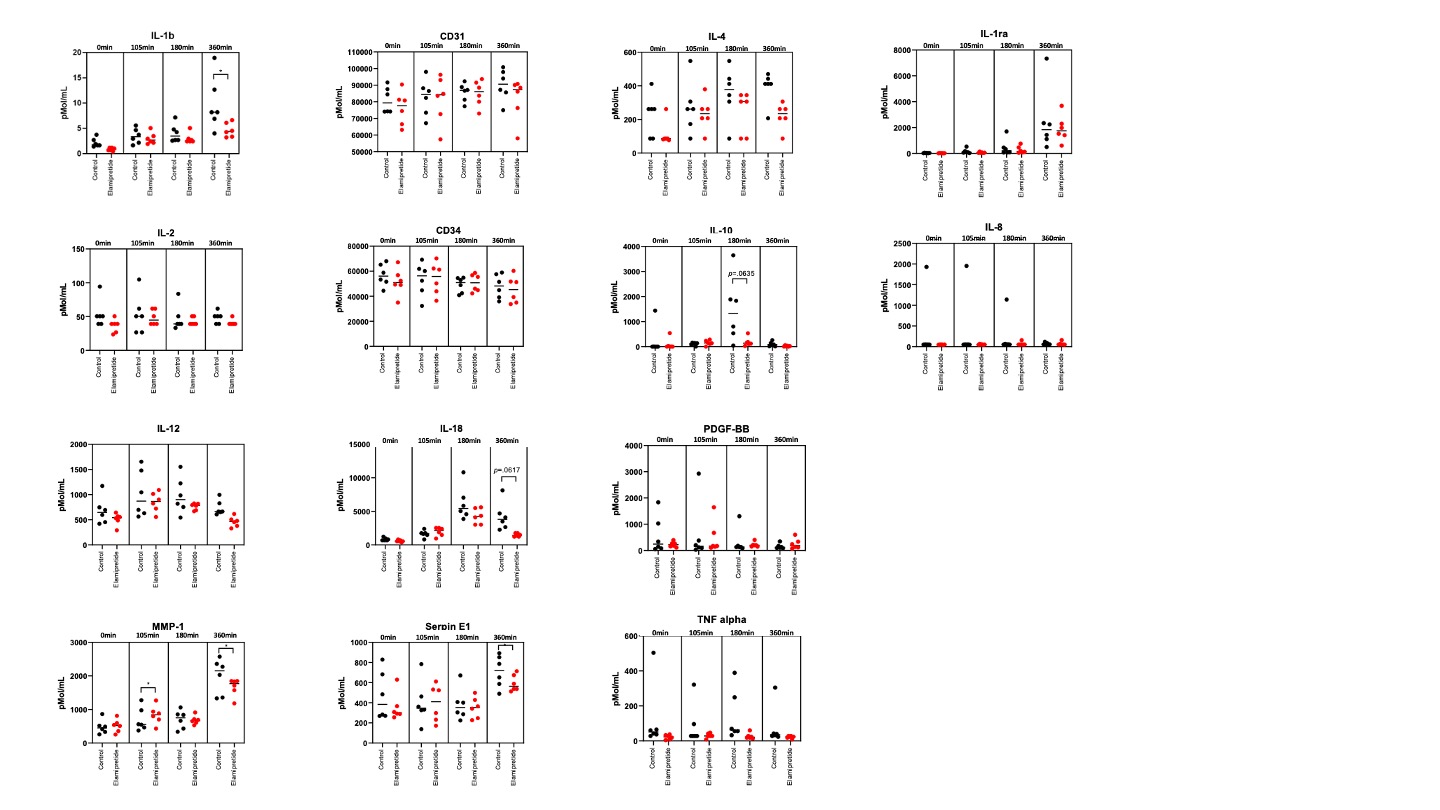
Early hemorrhagic shock resuscitation with primarily saline-based regimens is linked to greater mortality, reduced cardiac output, and cardiac dysfunction [46]. Large-volume crystalloid resuscitation can lead to many complications, or resuscitation injuries, to various organs, such as the kidney, liver, and intestinal tract [5, 6, 47]. It promotes cell edema, dysfunction, and, ultimately, death [7, 46]. In a study using a rat model of hemorrhagic shock, overly aggressive fluid resuscitation induced hepatocellular injury [48]. Furthermore, they found excessively aggressive fluid resuscitation was no better than more conservative resuscitation approaches at correcting plasma lactate concentration and preserving renal function. Overall, the study showed that large-volume isotonic crystalloid resuscitation provided no overall survival benefit. Crystalloid resuscitation and the associated dilution of coagulation factors also perpetuate the dysregulated coagulation state often observed after severe trauma [9–11]. In fact, hemodilution is one of the six main precipitants of coagulopathy in trauma (tissue trauma, shock, hemodilution, hypothermia, acidemia, and inflammation) [49]. Large-volume crystalloid resuscitation promotes interstitial edema [8], a significant risk for abdominal compartment syndrome, a complication with a mortality rate > 50% [50]. Reducing fluid requirements (Fig. 4.B) will also benefit resuscitation in resource-limited environments such as remote rural areas or military environments. Based on our data, in an average 70 kg pig, Elamipretide reduced fluid requirements by 2.6 liters [1.8–4.4] liters. This reduction in fluid requirement may be due to preserved vascular motor tone. While the effects of Elamipretide on large arteries and peripheral arterioles have not been described, Elamipretide promotes blood flow to the brain via nitric oxide-mediated cerebromicrovascular dilation [51]. Since there was no difference in norepinephrine in conjunction with a reduction in fluid requirements, Elamipretide may preserve capillary integrity and vascular responsiveness to endogenous and exogenous vasopressors. This particular effect of Elamipretide may be attributed to mitochondrial function protection within vascular smooth muscle cells. It is also plausible that Elamipretide serves to maintain endothelial integrity via metabolic protection, reducing fluid losses in the tissue through capillary leakage. The reduction in interleukin 6 at the end of the experiment in the Elamipretide group might reflect inflammation mitigation or a direct effect of elamipretide on interleukin 6 expression. Other studies of REBOA in pigs have demonstrated an elevation in serum interleukin 6 concentration. [52–54], which correlated with injury severity in trauma patients [55]. Interleukin 6 expression is associated with tissue injury, especially to the liver, and is directly related to mitochondrial injury [56–58]. In reality, multiple mechanisms of action likely influenced different organ systems in ways that reduced the resuscitation requirements we observed.
In the specific context of REBOA as an adjunct for shock resuscitation, Elamipretide had protective effects on not only tissue beds below the level of occlusion but also upstream. Myocardial injury is a common sequela of REBOA and is likely related to increased work strain against increased afterload due to occlusion. This strain on the heart can be mitigated via partial occlusion [59] or pharmacological intervention with beta-blockers to protect cardiomyocytes and reduce myocardial work and oxygen demand [60]. In the present study, we established a different pharmacologic method to reduce myocardial injury with Elamipretide. This protective effect likely translated to improved myocardial function, leading to the observed hemodynamic homeostasis in the treatment group during the critical care phase with no difference in serum lactate concentration, despite a much smaller volume of crystalloids administered. Similarly, we observed a renal protection phenomenon as evidenced by a reduction in serum creatinine concentration. We believe this finding results from direct mitochondrial protection in the kidney, improved oxygen delivery to the kidney, or a combination of both.
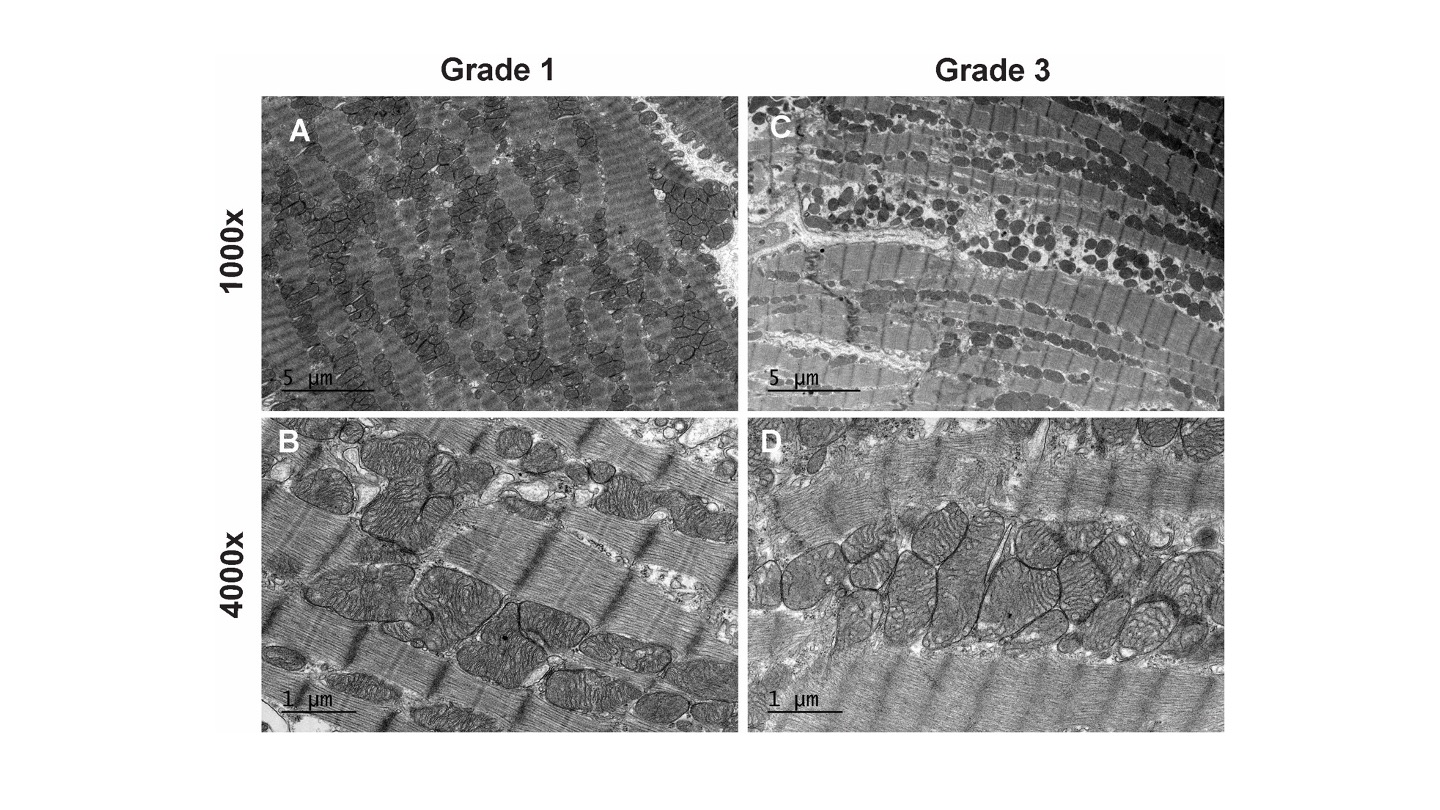
This study is subject to the limitations that characterize most large animal translational studies. First, we followed the animals for a limited duration, which may not be sufficient to replicate delayed complications observed in severely traumatized patients. This may also explain why the changes observed on histopathology and electron microscopy were not as pronounced as they might have been after a more extended study. Second, we performed a controlled hemorrhage without additional significant tissue damage; a polytrauma model (pulmonary contusion, long bone fracture, traumatic brain injury, burn, etc.) may reflect more realistic injuries such as those observed in patients who are so critically injured they require additional lifesaving maneuvers like REBOA.
Those limitations notwithstanding, the present data demonstrate that Elamipretide reduced fluid requirements and protected the heart and kidney in a pig model of hemorrhage and REBOA. Those benefits support our hypothesis that pharmacological interventions targeting mitochondria will likely benefit trauma patients with severe IRI. Future studies will focus on elucidating the mechanisms behind our observed benefits with a focus on cardiovascular and renal cellular metabolism as well as evaluating mitochondrial function in various tissue beds.
{kind=link}
{kind=link}
{kind=link}