According to the literature, musculoskeletal manifestations occur within two weeks or one month after diagnosis of COVID-19 to be accepted as COVID-related symptoms (6). Myalgia, arthralgia, arthritis, and fatigue are the most common musculoskeletal manifestations of COVID-19 infection. Rarely backache, myositis, neuropathies, and myopathies may also be considered (6, 26–28).
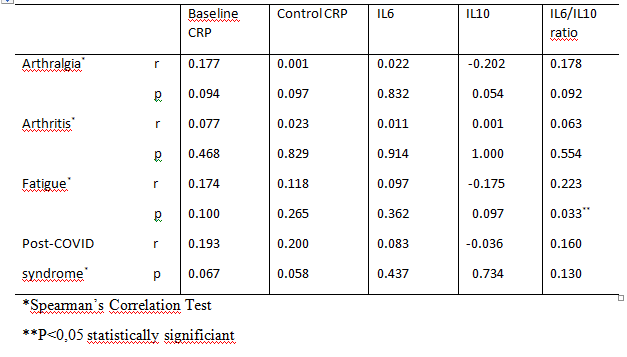
Cytokine response, muscle tissue damage, and increased lactate levels are possible mechanisms for myalgia; similarly, abnormal immune activation, complement activation, and immune complex deposition have been suggested as possible mechanisms responsible for arthralgia (29–31). Arthralgia may be reported as an initial or post-COVID symptom (32). It is less common than myalgia, and patients generally suffer from more severe pain (6). Although viral arthralgia has been described after well-known viral infections, it has also been frequently reported after COVID infection (6). Hoong et al. reported that 5.7% of 294 hospitalized COVID-19 patients had arthralgia. Arthralgia was revealed to not correlate with fever and pneumonia but was found to correlate with CRP levels (6). In this study, the rate of arthralgia was 34.8% (n = 38) in hospitalized COVID-19 patients and there was no correlation between basal CRP (r = 0.177, P = .094), control CRP (r = 0.001, P = .097), IL6 (r = 0.022, P = .832), and IL10 (r = 0-.202, P = .054) levels.
Autoimmune mechanisms play an important role in developing arthritis after COVID-19 infection. (8). In patients who develop joint pain following COVID-19 infection, post-COVID arthritis, rheumatic disease, or autoantibodies may be detected (8–11). Although reactive arthritis (12–16) is the most common rheumatic symptom after COVID-19 infection, other rheumatic conditions, such as rheumatoid arthritis or myositis, may be developed (17, 26, 27). Both mono-oligoarthritis may be detected, and large-small joint involvement may be revealed after COVID-19 infection (6). Taha et al. scanned 100 hospitalized COVID-19 patients and identified arthritis in 37% of them. The rate of arthritis was lower in the current study at 1.83% (n = 2). Although they found a statistically significant correlation between arthritis, CRP, and IL6 levels, there was no correlation between arthritis and basal CRP (r = 0.077, P = .023), control CRP (r = 0.023, P = .829), IL6 (r = 0.011, P = .914), and IL10 (r = 0.001, P = 1.000) levels in the current study.
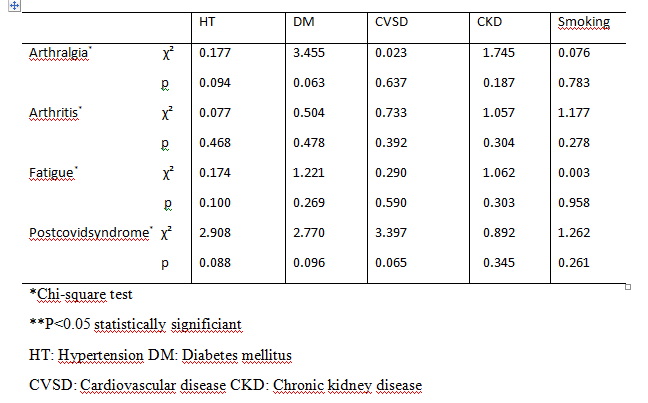
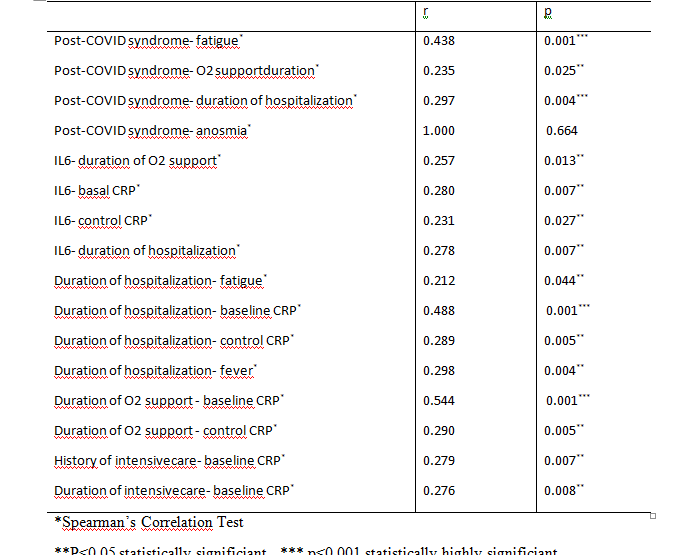
As symptoms persisted after active infection in some patients, the terms post-COVID and long COVID were developed. Symptoms of persistent fatigue, myalgia, depressive symptoms, and sleep disorders that occurred three months after COVID-19 were accepted as post-COVID syndrome symptoms (19). In a systematic review, 80% of patients were shown to have persistent symptoms for a week after infection (33). In two studies from Switzerland and Italy, 32% of outpatients and 83% of hospitalized patients had persistent symptoms (34, 35). In a United Kingdom-based survey, 20% of patients were shown to have these symptoms for five weeks, and 10% had these symptoms for 12 weeks (36). Additionally, data from a Google-based survey taken 6 ± 3 months after COVID-19 infection (n = 616)showed that 30.7% of individuals met fibromyalgia criteria because of persistent symptoms(37). Co-morbidities were revealed as risk factors for post-COVID syndrome, but there was no association between post-COVID syndrome and co-morbidities in the current study. Laboratory parameters such as lymphopenia, thrombocytopenia, elevated D-dimer, LDH, troponin, elevated CRP, ferritin, and IL6 were revealed as predictive factors for post-COVID syndrome (36). Ortelli et al. compared 12 COVID-positive patients with healthy controls and showed more fatigue, cognitive dysfunction, apathy, and executive dysfunction in COVID-positive patients. They also observed elevated IL6 levels and hyper-inflammation in these patients (20). In the current study, there was no correlation between post-COVID syndrome and basal CRP levels (r = 0.193, P = .200) or control CRP levels (r = 0.067, P = .058). Additionally, fatigue (r = 0.438, P = .001), duration of hospitalization (r = 0.297, P = .004), and duration of O2 support (r = 0.235, P = .025) were positively correlated with post-COVID syndrome. In a review, abnormal inflammation and IL6/IL10 imbalance were revealed to play a role in post-COVID syndrome(21). In the current study, there was no correlation between IL6 (r = 0.083, P = .437), IL10 (r = 0-.036, P = .734), the IL6/IL10 ratio (r = 0.160, P = .130), and post-COVID syndrome. It has been suggested that COVID-19 infection can cause lymphatic blockage, and there may be an association between post-COVID syndrome and anosmia. However, there was no correlation between post-COVID syndrome according to the current study (r = 01.000, P = .664).
CRP is a non-specific acute-phase protein that increases during inflammation, infection, and tissue damage. In addition, CRP levels increase during inflammatory responses induced by IL6. Therefore, CRP and IL6 are expected to increase in acute-phase reactions together (38). In addition, Liu et al. suggested that IL6, CRP, and procalcitonin levels may have a prognostic role in COVID-19 infection (39). Coomes et al. indicated that IL6 levels were higher in severe COVID-19 patients (40). In the current study IL6 levels were positively correlated with basal CRP levels (r = 0.280, P = .007), control CRP levels (r = 0.231, P = .027), O2 support duration (r = 0.257, P = .013), and hospitalization duration (r = 0.278, P = .007). Baseline CRP levels were positively correlated with O2 support duration (r = 0.544, P = .001), hospitalization duration (r = 0.488, P = .001), history of intensive care (r = 0.279, P = .007), and duration of intensive care (r = 0.276, P = .008). Control CRP levels were positively correlated with O2 support duration (r = 0.290, P = .005) and hospitalization duration (r = 0.289, P = .005). These results support the hypothesis that IL6 and CRP levels may have a prognostic role in COVID-19 patients. Kappleman et al. determined IL6 level as a predictor for post-COVID syndrome (41). In the current study, there was no correlation between IL6 levels and post-COVID syndrome (r = 0.083, P = .437).
IL10 has immunosuppressive functions and is produced by various cells like monocytes, macrophages, dendritic cells (DCs), mast cells, eosinophils, neutrophils, natural killer cells, B cells, and T cells. It has been shown that IL10 and IL6 levels increase together in COVID-19 infection. It has been suggested that increased levels of IL10 may be associated with cytokine storms, poor prognosis, and complications (42). However, in the current study, there was no correlation with IL6 levels (r = 0.180, P = .085), intensive care history (r = 0.063, P = .550), intensive care duration (r = 0.061, P = .564), hospitalization duration (r = 0-.129, P = .221), or O2 support duration (r = 0-.148, P = .158).
As there was no correlation between musculoskeletal manifestations, post-COVID syndrome, baseline or control CRP, IL6, and IL10 levels, further studies are needed to understand the mechanisms of symptoms in COVID-19 infection. The main limitations of this study are the small sample size and inclusion of only hospitalized patients. There should be multicenter, and outpatient populations included in studies with larger sample sizes. If correlations between these parameters are detected, new follow-up strategies may be developed.
{kind=link}
{kind=link}
{kind=link}