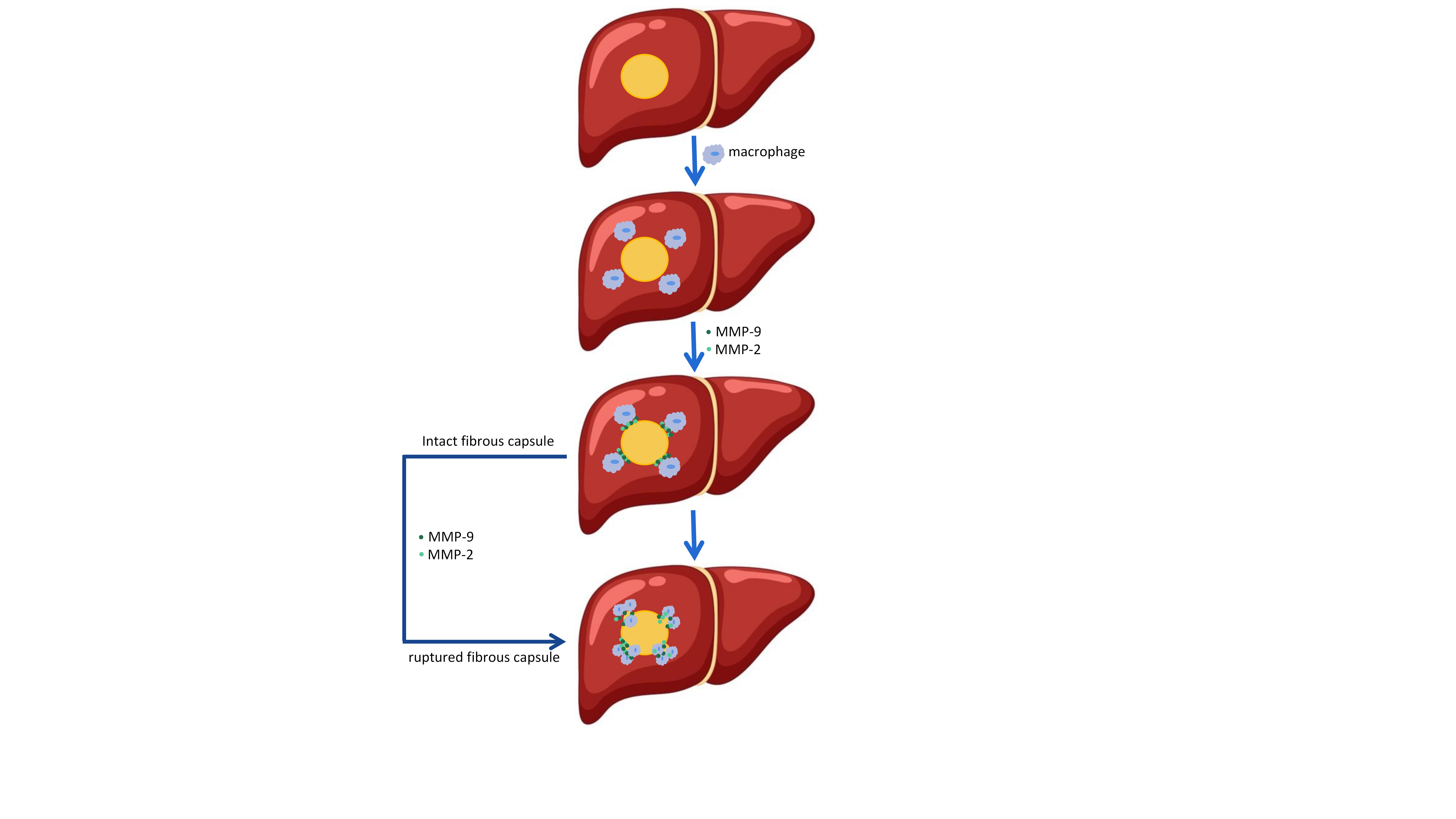
We hypothesized that macrophages destroyed the HCC fibrous capsule by secreting MMP-9/MMP-2, leading to invasion and metastasis of HCC. In this study, validation by immunohistochemistry and immunofluorescence showed that a significant number of macrophages and their derived MMP-9/MMP-2 aggregates in the area of the ruptured FC. Next, western blot analysis and Quantitative real-time PCR proved the high expression of MMP-9/MMP-2 in the area of the ruptured FC. Finally, MMP-9/MMP-2 were able to discriminate effectively between ruptured FC and intact FC were verified by ELISA. Hence, our finding reveals that macrophage-derived MMP-9/MMP-2 are closely related to the rupture of the FC of hepatocellular carcinoma leading to tumor invasion.
3.1 FC rupture is significantly correlated with vascular invasion, TNM stage, AFP, and tumor recurrence
The different HCC Patients with ruptured FC (n = 26) and intact FC (n = 19) were included in this study. Overall, ruptured FC patients and intact FC patients were well matched for age and sex (P = 0.863 and P = 1.000, respectively). Table 1 shows the clinicopathological data of all the patients. We retrospectively analyzed the clinicopathological data of all the patients, using Chi-Squared Test (χ2) to calculate the possible correlation between whether the FC was ruptured or not and the clinicopathological data, and a P value < 0.05 was considered statistically significant. There were significant correlations observed between the ruptured FC and vascular invasion (P = 0.0006), TNM stage (P = 0.021), AFP (ng/ml) (P = 0.0033), and recurrence (P = 0.036), which could guide the clinical therapy.
Table 1:clinical features of patients (n = 45)
|
Variables
|
Repured FC (n=26)
|
|
Intact FC(n=19)
|
|
P value
|
|
Age(years), mean ± SD
|
57.92±12.73
|
|
57.32 ±10.09
|
|
0.863
|
|
Gender,n(%)
|
|
|
|
|
|
|
1.000
|
|
Male
|
24
|
92.31%
|
|
17
|
89.47%
|
|
|
|
Female
|
2
|
7.69%
|
|
2
|
10.53%
|
|
|
|
Hepatitis virus status, n (%)
|
|
|
|
|
|
|
0.029
|
|
HBsAg (+)
|
25
|
96.15%
|
|
14
|
73.68%
|
|
|
|
HBsAg (-)
|
1
|
3.85%
|
|
5
|
26.32%
|
|
|
|
ALT (IU/L), n (%)
|
|
|
|
|
|
|
0.138
|
|
>40
|
12
|
46.15
|
|
13
|
68.42%
|
|
|
|
≤40
|
14
|
53.85%
|
|
6
|
31.58%
|
|
|
|
AST (IU/L), n (%)
|
|
|
|
|
|
|
0.463
|
|
>35
|
15
|
57.69%
|
|
13
|
68.42%
|
|
|
|
≤35
|
11
|
42.31%
|
|
6
|
31.58%
|
|
|
|
CEA(ng/ml)
|
|
|
|
|
|
|
0.365
|
|
>5
|
4
|
15.38%
|
|
5
|
26.32%
|
|
|
|
≤5
|
22
|
84.62%
|
|
14
|
73.68%
|
|
|
|
CA19-9(U/ml)
|
|
|
|
|
|
|
0.467
|
|
>27
|
8
|
30.77%
|
|
4
|
21.05%
|
|
|
|
≤27
|
18
|
69.23%
|
|
15
|
78.95%
|
|
|
|
CA125(U/ml)
|
|
|
|
|
|
|
0.103
|
|
>35
|
6
|
23.08%
|
|
1
|
5.26%
|
|
|
|
≤35
|
20
|
76.9%
|
|
18
|
94.74%
|
|
|
|
AFP(ng/ml)
|
|
|
|
|
|
|
0.033
|
|
>400
|
12
|
46.15%
|
|
3
|
15.79%
|
|
|
|
≤400
|
14
|
53.85%
|
|
16
|
84.21%
|
|
|
|
Vascular invasion, n (%)
|
|
|
|
|
|
|
0.006
|
|
No
|
15
|
57.69%
|
|
18
|
94.74%
|
|
|
|
Yes
|
11
|
42.31%
|
|
1
|
5.26%
|
|
|
|
Differentiation,n (%)
|
|
|
|
|
|
|
0.063
|
|
Well or moderately
|
17
|
65.38%
|
|
17
|
89.47%
|
|
|
|
Poorly
|
9
|
34.62%
|
|
2
|
10.53%
|
|
|
|
TNM Stage,n (%)
|
|
|
|
|
|
|
0.021
|
|
I
|
15
|
57.69%
|
|
18
|
94.74%
|
|
|
|
II
|
10
|
38.46%
|
|
1
|
5.26%
|
|
|
|
III, IV
|
1
|
3.85%
|
|
0
|
0%
|
|
|
|
Recurrence
|
|
|
|
|
|
|
0.036
|
|
Yes
|
19
|
73.08%
|
|
8
|
42.11%
|
|
|
|
No
|
7
|
26.92%
|
|
11
|
57.89%
|
|
|
3.2 Hepatocellular carcinoma cells can invade the paracancerous liver tissue through the ruptured area of FC
To validate the route of the tumor invasion to the paracancerous liver tissue, we retrospectively collected Magnetic resonance imaging (MRI) data from HCC patients (n = 6), and the results showed that hepatocellular carcinoma cells directly migrated into the paracancerous liver tissues through the ruptured area of FC and then displayed invasion (Fig. 2A). In contrast, HCC cells from intact FC patients were wrapped up in intact FC without contacting the paracancerous liver tissue due to the restriction of FC (Fig. 2B). To further demonstrate our finding, we performed H&E staining on the tissue slides of HCC patients (n = 6), and the above phenomenon was noted in their corresponding HE stained slides (Fig. 2C, D). Taken together, these data suggested that FC rupture is a precondition for HCC cell invasion and metastasis.
3.3 Macrophages are related to FC rupture
To verify whether macrophages and HSCs are correlated with FC rupture, we used COL1A1 immunohistochemical staining to identify the location of ruptured and intact FC, and CD163 and α-SMA immunohistochemical staining of the ruptured as well as intact area of FC were performed on all the serial slides (n = 6). The results indicated that the ruptured area of FC (Fig. 3A) and the intact area of FC (Fig. 3D) were identified by immunohistochemical staining in COL1A1, ruptured FC had a higher CD163 and α-SMA-positive rate than intact FC (Fig. 3B, C, E, F). It indicated that CD163 and α-SMA expression were associated with FC rupture. To further illustrate that macrophages and HSCs are related to FC rupture, the expression of CD163 and α-SMA were analyzed by Image J software, then statistical analysis was conducted using GraphPad Prism (version 8.0) software programs, which showed that the expression of CD163 in the ruptured area of FC was significantly higher than that in the intact area of FC (P = 0.0015)(Fig. 3G), while α-SMA was not correlated (P = 0.6778)(Fig. 3H). The above results indicated that the macrophages were massively aggregated in the ruptured FC area and directly associated with FC rupture, whereas activated HSCs expressing α-SMA could not be correlated with FC rupture. To sum up, macrophages are correlated with FC rupture.
3.4 MMP-9/MMP-2 is critical molecule that lead to FC rupture
First, we still used COL1A1 immunohistochemical staining, the ruptured area of FC (Fig. 4A) and intact area of FC (Fig. 4D) were demonstrated by COL1A1 immunohistochemical staining. To validate whether MMP-9/MMP-2 were related to FC rupture, we performed MMP-9 and MMP-2 immunohistochemical staining on all the serial slides. The result indicated that the expression of MMP-9 in the ruptured FC patients was significantly higher than in the intact FC patients (P = 0.0196) (Fig. 4B, E) and the expression of MMP-2 in the ruptured FC patients was also significantly higher than in the intact FC patients (P = 0.0453) (Fig. 4C, F). In order to further verify that MMP-9/MMP-2 is related to FC rupture, the expression of MMP-9/MMP-2 was analyzed by Image J software, then statistical analysis was conducted using GraphPad Prism (version 8.0) software programs, the results suggest that MMP-9/MMP-2 is indeed correlated with FC rupture (Fig. 4G, H). In addition, the expression of MMP-9/MMP-2 in the ruptured area of FC was significantly higher compared to that in the relatively intact area of the same ruptured FC patients (P = 0.0059/P = 0.0481) (Fig. 4I, J).
To further investigate the above views, we further conducted western blot analysis of the ruptured area of FC and its relatively intact area of FC (RIFC) in 7 patients with ruptured FC. The findings indicated that the levels of MMP-9/MMP-2 proteins in the ruptured area of FC were significantly higher than those in the RIFC (Fig. 4K, L, M). Next, we confirmed these changes in mRNA levels by doing qRT-PCR, the data indicated that MMP-9/MMP-2 expression was significantly indeed higher in the FC rupture area than in the RIFC area(Fig. 4N, O, P). In summary, MMP-9/MMP-2 is related to FC rupture and is the critical molecule that causes FC rupture.
3.5 MMP-9/MMP-2 is derived from macrophages causing FC rupture
To verify whether MMP-9/MMP-2 is derived from macrophages, we performed immunohistochemical staining and immunofluorescence staining on the ruptured area of FC (all serial slides), we found that CD163 and MMP-9/MMP-2 were both abundantly expressed in the ruptured area of FC in the consecutive slides (Fig. 5A, B, C). Interestingly, in the ruptured area of FC, the area that expressed CD163 was identical to MMP-9/MMP-2, this is indicative of the colocalization of CD163 with MMP-9/MMP-2. Furthermore, we conducted CD163/MMP-9/MMP2 co-immunofluorescence staining to validate this observation. The results indicated that there were substantial co-localizations of CD163 with MMP-9 and MMP-2 (Fig. 5D, E) in the ruptured area of FC. Based on the above results, it was concluded that a significant number of macrophages aggregated in the ruptured area of FC and their derived MMP-9/MMP-2 is correlated with FC rupture as well as tumor invasion.
3.6 Clinical diagnostic value of MMP-9/MMP-2 for FC rupture
To determine the potential diagnostic value of MMP-9/MMP-2 for FC rupture or not, the protein concentrations were measured by ELISA in the ruptured (n = 19) and intact FC tissues(n = 19). All ELISA data was then analyzed with Prism software 8.0 (GraphPad Software) and cutoff values were calculated with SPSS 26.0 (IBM; USA). The results demonstrated that the expression of MMP-9 in the ruptured FC tissues was significantly higher compared to intact FC tissues (P = 0.0156) (Fig. 6A), and the expression of MMP-2 in the ruptured FC tissues was significantly higher than intact FC tissues (P = 0.0267) (Fig. 6B), this further validated the observation that MMP-9/MMP-2 is correlated with FC rupture.
Furthermore, the ROC curve was used to determine the diagnostic value of MMP-9/MMP-2 for FC rupture depending on the tissue MMP-9/MMP-2 protein concentration. The optimal cutoff value for MMP-9 was 27007.56ng/g, with a sensitivity of 63.2% and specificity of 89.5%, and MMP-9 showed an AUC of 0.817 for discriminating ruptured FC from intact FC(Fig. 6C). The optimal cutoff value for MMP-2 was 1622.70ng/g, with a sensitivity of 89.5% and specificity of 57.9%, and MMP-2 showed an AUC of 0.795 for discriminating ruptured FC from intact FC (Fig. 6D). In conclusion, MMP-9/MMP-2 was able to discriminate effectively between ruptured FC and intact FC, suggesting great potential as a diagnostic for FC rupture or not. These values had important implications for efforts to pre-diagnose the rupture of FC in HCC patients and prevent a recurrence.
{kind=link}