The extent of resection for non-metastatic splenic flexure colon cancer chosen by the surgeon is often empirically supported rather than based on evidence[13]. Extended procedures are the most common surgical treatments so far for splenic flexure colon cancer[14], and have been recommended to overcome the poor oncologic outcomes observed in patients with splenic flexure colon cancers[15]. One survey fielded on this topic showed that ERHC was the most preferred procedure by 63% of those surveyed followed by LHC (23%) and segmental resection (14%) in the United Kingdom[16]. In China, our recent survey revealed that the most preferred procedure for splenic flexure colon cancer was LHC or Extended LHC (97.4%), followed by segmental resection (1.8%) and ERHC (0.9%) (manuscript not published). Interestingly, increased adoption of segmental resection for the treatment of non-metastatic splenic flexure colon cancer as the year progresses was observed in the present study.
For short-term outcomes, compared to a formal left hemicolectomy, a segmental resection was reported to be associated with a shorter operative time with equivalent post-operative morbidity based on the analysis of the ACS-NSQIP colectomy-targeted database[17]. Our previous network meta-analysis revealed that ERHC was associated with a higher risk of postoperative ileus but a non-significant trend for lower anastomotic dehiscence when compared with more restricted resections[12]. However, the evidence in the literature regarding the long-term oncological advantages of extended resection over segmental resection is sparse. A nationwide retrospective cohort study including 1304 cases showed that segmental resection and extended procedures (extended right and left colectomies) had comparable survival rates (5-year OS 84% vs. 83%, 5-year progression-free survival 85% vs. 84%)[18]. In fact, our study is the largest study to date to compare survival between segmental resection and extended procedure. Our initial analysis of baseline characteristics showed that extended resection was more frequently applied in advance-stage tumors, which was probably the reason why extended resection was associated with a slightly lower 5-year CSS rate. This hypothesis was confirmed by the re-comparison of the survival after the PSM or subgroups analysis of locally advanced stage tumors (stage III or tumor size ≥ 7 cm). The results of the re-comparison revealed that both the 5-year CSS and 5-year OS rates in the extended resection group and segmental resection group were comparable. Moreover, while the numbers of harvested lymph nodes increased in the extended resection group the numbers of invaded lymph nodes remained relatively constant between groups. This fact together with the previous indications suggested that extended procedures have no statistically significant oncological benefits over a less aggressive approach of segmental resection. Segmental resection seems an effective alternative for splenic flexure tumors, even for non-metastatic locally advanced cases.
It is noteworthy that the difference in the survival estimates among various extended procedures, including STC, ERHC, and LHC, was not analyzed due to a lack of grouping data in the SEER database. Several previous studies with small sample sizes showed no differences among various procedures. Bademci et al.[9] found that STC, LHC, and segmental resection had similar long-term survival by including 124 cases. A previous study included 170 patients by Arévalo et al.[19] showed that ERHC and LHC had comparable OS and DFS in the treatment of splenic flexure colon cancer using PSM. Thus, further studies are warranted to define the role of various extended procedures for splenic flexure colon cancer.
Interestingly, in the present study, we found a potential link between a later year of diagnosis and improved CSS over 2000–2018. From a population-based perspective, an increased rate of harvested lymph node count ≥ 12 or ≥ 11 observed over this 18-year period might be the underlying reason. Stocchi et al.[20] found that harvest of at least 12 nodes was related to surgery after 1991 (85% vs 69%, P < 0.001) in stage II colon carcinoma. Since the 12-node minimum rule was first proposed in 1990[21], this fact together with the positive link indicated that it is of great importance to understand and determine the optimal cutoff for the number of lymph nodes needed for surgery of non-metastatic splenic flexure colon cancer.
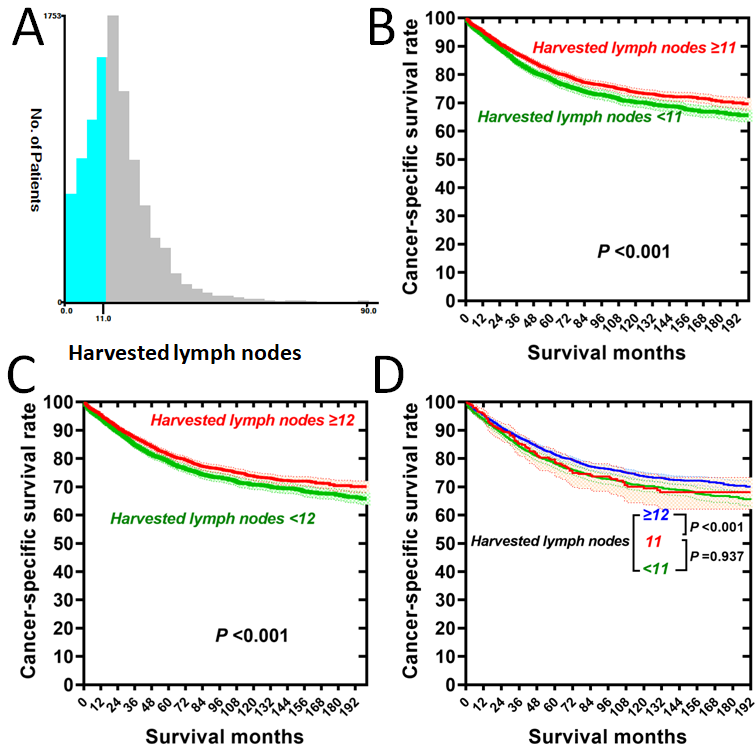
Besides the detection of involvement, the number of harvested lymph nodes itself has prognostic relevance in stage colorectal II/III cancers[22]. However, the exact relationship between the examined lymph node count and CSS at the time of resection for non-metastatic splenic flexure colon cancer is still ill-defined. In addition, although the 12-node minimum has been recognized as a consensus standard for surgical performance for colorectal cancer[23], this threshold was met only in about three-quarters of cases (85% for right colon carcinomas and 72% for left colon carcinomas[20]). It is known that the number of harvested lymph nodes was related to surgery over time, colon tumor location (right colon or left colon), individual surgeon, and length of specimen[20]. Thus, the 12-node standard for the total number of lymph nodes may not be equally applicable in all cancer locations. At least two previous studies fielded on this topic had proposed a lower threshold of 11 to be the optimum number of harvested lymph nodes for left-sided colon cancer[7, 24]. In the present study, the analysis of population-level data showed that no difference regarding 5-year CSS between patients with < 11 lymph nodes harvested and patients with 11 lymph nodes harvested were found, while significant CSS difference was observed between patients with 11 lymph nodes harvested and patients with ≥ 12 lymph nodes harvested. Thus, we confirmed the optimum threshold of 12 for the harvested lymph node count during non-metastatic splenic flexure colon cancer surgeries. On the other hand, larger numbers of harvested lymph nodes in the extended resection did not confer any additional benefit relative to segmental resection with regard to CSS, probably due to no increase in the resected invaded lymph node numbers in the present study. Thus, understanding the distribution of metastatic lymph nodes and the different anatomies for non-metastatic splenic flexure colon cancer might be essential. For instance, the inferior mesenteric artery lymph node was routinely resected during LHC while might normally have been left behind in ERHC and segmental resection in China. Our recently published study analyzed a single-center experience of 117 consecutive non-metastatic splenic flexure colon cancer surgeries performed over a period of 7 years and observed no metastatic lymph nodes at the root of the inferior mesenteric artery[25], which is similar to a previous study observed by Nakagoe et al.[26] Consequently, It might not be necessary to resect the inferior mesenteric artery lymph node during non-metastatic splenic flexure colon cancer surgery.
The strength of this study lies in the large patient numbers, even for relatively rare colon cancer of splenic flexure, and long follow-up time, which indicates the almost real-world outcomes and might be a powerful resource for identifying gross trends. However, there are several limitations of this study. First, confusing nomenclature as well as the uncertainty in exact surgical extent are common in the literature regarding colectomy for splenic flexure colon cancer[27]. Secondly, our study was a retrospective data analysis and therefore subject to the limitation common to this research. However, the PSM was performed to adjust for confounding factors and to overcome potential selection bias. Thirdly, like all registry studies based on the SEER database, more detailed information about oncological outcomes, including tumor recurrence sites, was not provided. This issue warrants further investigation in cohorts with detailed oncological outcomes data.
{kind=link}
{kind=link}