ADIC levels can undergo alterations via a variety of mechanisms in T2DM, which may also differ markedly from those in healthy individuals [6]. Conversely, alterations in ADIC secretion can change the pathophysiology and progression of T2DM [15]. Increasing evidence has indicated that alterations in ADIC levels may be the major biochemical mediators contributing to the pathophysiology of inflammatory and metabolic diseases, including T2DM [16]. Accordingly, ADICs represent an increasingly promising therapeutic target for T2DM treatment. In this post-hoc study of the CONFIDENCE clinical trial, we found that the levels of IL-1β and IFN-γ, the pro-inflammatory cytokines, were notably decreased after treatment with exenatide, whereas the opposite trend was seen in the insulin treatment group. However, no significant changes were detected in the levels of the adipokines leptin and FGF21 in any of the intervention groups. Significant differences in ΔIL-1β and ΔIFN-γ were seen between treatment groups. Additionally, we found that changes in ADIC contents might contribute to the differences in changes in metabolic factors, IR, and β-cell function among the three groups. To the best of our knowledge, relatively few studies have compared changes in both adipokine and inflammatory cytokine levels while also investigating the associations of metabolic factors, glycemic indices, β-cell function, and ADIC levels with different hypoglycemic agents.
There is abundant evidence supporting that chronic inflammation, marked by increased levels of inflammatory cytokines, plays a crucial role in the pathophysiology of T2DM. However, the mechanisms are still not fully understood [17–19]. Increased concentrations of circulating inflammatory cytokines may augment the risk of metabolic disorders as well as increase pancreatic islet macrophage infiltration and apoptosis of β cell. And these effects may eventually contribute to the development of T2DM [20–22]. The inflammatory cytokines IL-1β and IFN-γ are key pro-diabetic inflammatory risk factors [23]. The levels of both IL-1β and IFN-γ are increased in animal models of T2DM, and both factors can impair insulin signaling, induce β-cell apoptosis and dysfunction, and promote IR [24, 25]. Results in previous studies showing a significant correlation between IL-1β and IFN-γ suggested their close interaction[24, 25]. Theoretically, the inhibition of inflammation, accompanied by a reduction in inflammatory cytokine levels, may lead to an improvement in metabolic parameters and β-cell function in T2DM and the amelioration of the associated complications. Accordingly, recent studies have assessed the potential of IL-1β and IFN-γ as novel therapeutic targets in the treatment of T2DM [26, 27]. Some hypoglycemic agents have been reported to possess anti-inflammatory characteristics. Studies have consistently shown that intervention with GLP-1 agonists leads to significant reduction of circulating IL-1β and IFN-γ [28], and these anti-inflammatory effects were recapitulated with exenatide intervention in our study. Similar reductions in IL-1β and IFN-γ contents were not observed in the insulin and pioglitazone treatment groups. However, reports on the effects of insulin treatment on inflammatory cytokine levels have been inconsistent. For instance, Aas et al found that the serum levels of high-sensitivity C-reactive protein (hs-CRP) and tumor necrosis factor alpha (TNF-α) were significantly increased after neutral protamine Hagedorn (NPH) insulin intervention [29], whereas the opposite result was reported in the most recent study [30]. Different characteristics of the participants, different effects on body weight or different insulin regimens may explain these discrepant findings. In the present study, we found that IL-1β and IFN-γ levels increased in the group receiving premixed insulin treatment, indicating that insulin, even though it has the strongest hypoglycemic effects of the three agents tested, may play a pro-inflammatory role with long-term administration. This pro-inflammatory effect may offset the benefit of lowering blood glucose. It could partly explain the non-reduction in the number of major adverse cardiovascular events after insulin treatment, even though glucose levels within the target range were achieved [31]. Studies investigating the effects of pioglitazone on IL-1β and IFN-γ are scarce. Here, we found that the levels of circulating IL-1β and IFN-γ decreased in the exenatide group, but not in the pioglitazone group. The accompanying reduction in weight and waist circumference observed in the exenatide group, but not the other two groups, may explain this difference. In addition, in the ANCOVA analysis, after controlling for the effect of baseline, body weight, and HbA1c, changes in IL-1β and IFN-γ contents in the exenatide group were significantly greater compared with those in both the insulin and pioglitazone groups. These results further confirmed the anti-inflammatory characteristics of exenatide. Results in the present study demonstrated that exenatide could exert both anti-hyperglycemic and anti-inflammatory effects on diabetes, and its anti-inflammatory effects were superior to those of insulin and pioglitazone, regardless of the changes in body weight and HbA1c.
We further found that ΔLgIL-1β was independently associated with Δweight, ΔBMI, and ΔLgHOMA-IR in the multiple linear regression analysis. These findings suggested that the changes in weight, BMI, and IR were associated with changes in IL-1β levels. However, this association was lost when the effects of the antidiabetic agents were controlled for, implying that IL-1β might play an intermediate role between changes in weight, BMI, HOMA-IR, and antidiabetic agents (mainly exenatide). Exenatide treatment may contribute to a decrease in IL-1β levels along with a reduction in body weight, BMI, and HOMA-IR in this group. However, no associations were found among glycemic indices, β-cell function, and ADIC contents. Our findings suggested that in consideration of weight and IR in T2DM, the anti-inflammatory characteristic of agents should be considered when choosing hypoglycemic agents.
The discovery of leptin, the first adipokine to be identified, was considered a milestone in adipokine research [32. 33]. Leptin has an important role in the regulation of satiety, energy expenditure [34], β-cell mass, insulin sensitization, and atherogenesis [35]. A recent study reported that, among the assessed adipocytokines, leptin was found to be the hub of the biomarker correlation network in T2DM [36]. Elevated leptin levels in T2DM have been reported to be associated with the progression of diabetic complications through its stimulatory effects on oxidative stress and inflammation [37, 38]. Numerous studies to date have investigated the effects of leptin replacement therapy on IR and hyperglycemic management in animal models of diabetes; however, relatively few studies involved in the investigation on alteration of leptin after medical treatment. Metformin and DDP-IV have been reported to decrease leptin levels in T2DM patients [7]. Nevertheless, data regarding the effects of GLP-1 on leptin levels in T2DM remain limited. Frøssing et al found that liraglutide treatment in women with PCOS resulted in a significant reduction in the leptin level [39]. Moreover, a different study recently reported that treatment with a combination of metformin and exenatide promoted a reduction in leptin levels in patients with both obesity and T2DM [40]. The mean BMI of participants in that study, however, was greater than 31 kg/m2, which was significantly higher than the BMI (25 kg/m2) observed in our study. This might explain the discrepancy between the two studies regarding leptin levels. Reports of the effect of pioglitazone on the leptin level in T2DM have also been contradictory [41], while studies assessing the effect of insulin on leptin levels have been rare. In the present study, the leptin level was not altered in any of the intervention groups, and no differences in changes in leptin levels were observed among the three treatments. Our findings suggested that regular hypoglycemic agents did not affect the leptin level in non-obese diabetic population. Given the limited effect of exogenous leptin treatment on diabetes [42], leptin may not be a good marker or target for the treatment of hyperglycemia regarding this lean group of patients.
FGF21, an adipokine predominantly expressed in the liver, stimulates glucose uptake into adipocytes, promotes an increase in energy expenditure, and improves glucose and lipid metabolism [43]. Patients with T2DM have increased FGF21 levels and decreased expression of FGF receptors resulting from a so-called ‘FGF21-resistant state’ [43]. Studies have shown that the administration of FGF21 can exert anti-metabolic and anti-diabetic effects in T2DM [44]. Accordingly, regulating the circulating level of FGF21 might enhance its anti-diabetic effects in T2DM and eventually reduce diabetic complications. However, conflicting results have been reported for the effects of hypoglycemic agents on FGF21. Li et al demonstrated that fasting plasma FGF21 concentrations were decreased after treatment with rosiglitazone in poorly managed T2DM, in contrast to that reported for db/db mice by Muise et al [45, 46]. In patients with T2DM, treatment with a GLP-1 receptor agonist led to a decrease in FGF21 levels [47]. However, no investigation to date has evaluated the effect of insulin on FGF21 expression in diabetes. In the present study, FGF21 levels did not significantly change in newly diagnosed patients with any of the treatments assessed. As FGF21 plasma concentrations exhibited high inter-individual variability (0.05 to 5.5 ng/mL) in healthy individuals [48], we speculated that variability in FGF21 plasma concentrations might also influence the detection of FGF21 in patients with diabetes, which might partially explain the discrepancies between ours and previous studies. In addition, compared with previous studies, the patients in our study were all newly diagnosed, relatively lean, and had lower HbA1c, which might also contribute to the different results obtained. Given its high inter-individual variability and the results in our study, FGF21 may have limited value for clinical use. However, the effects of other hypoglycemic agents on this adipokine need to be investigated to better determine its diagnostic and therapeutic value in diabetes.
Interestingly, during the analysis, we also found a correlation between a reduction in adipokine levels and that in the concentrations of inflammatory cytokines. A strong positive correlation was observed between plasma and adipose tissue levels of hs-CRP, leptin, and TNF-α.Here, we concluded that there was a strong relationship between adipocytokines and inflammatory markers, suggesting that cytokines secreted by adipose tissue play a role in the increased secretion of inflammatory proteins by the liver [49]. The findings of the present study indicated that adipokines and reduced levels of inflammatory cytokines had an interactional effect in the condition of hyperglycemia. Accordingly, we assessed adipokine and inflammatory cytokine content together in the present study.
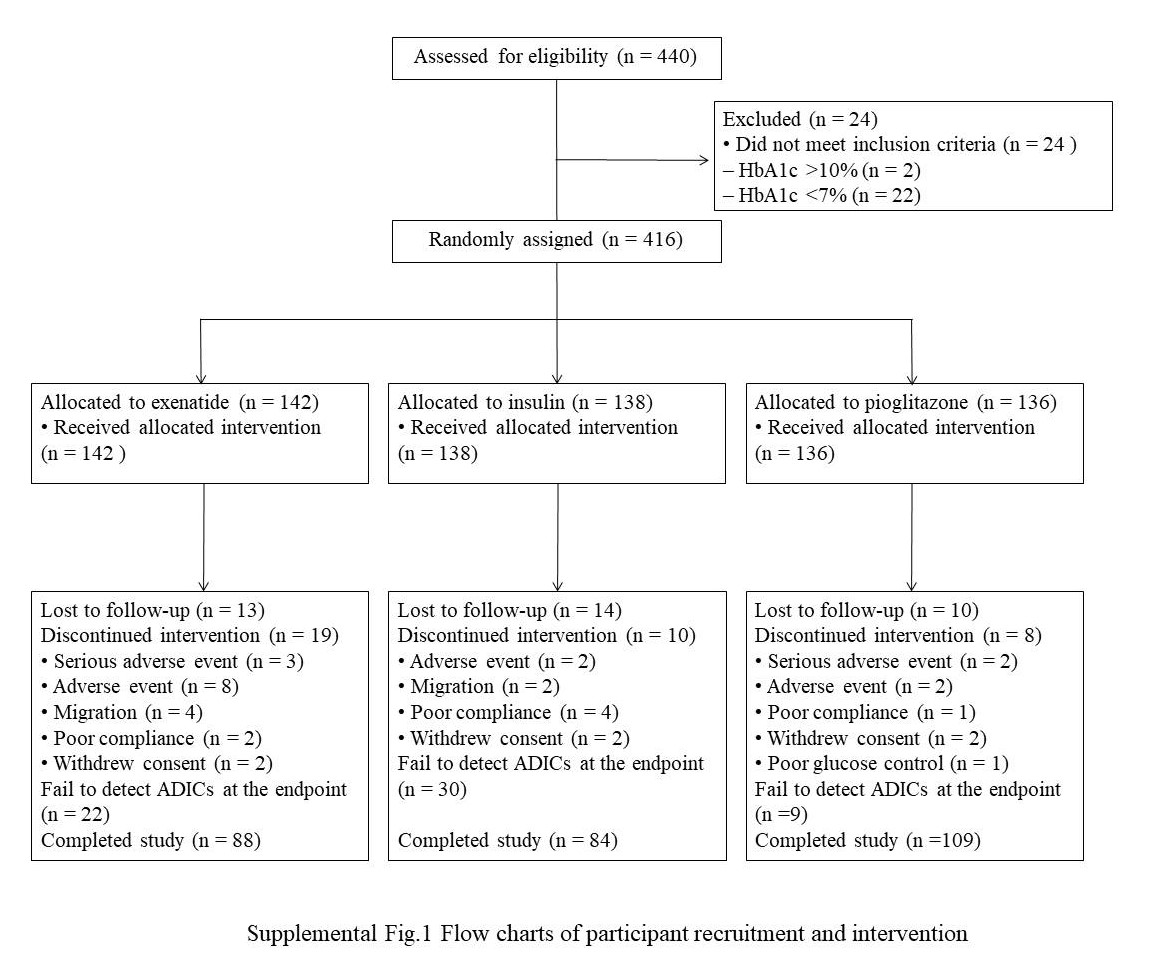
One limitation of this study was that metformin was not included in the analysis as this was a post-hoc study of the CONFIDENCE trial. However, we believe that patients without previous treatment or the confounding effects of other hypoglycemic agents would allow for a better comparison of treatment with the three agents on changes in ADIC levels. In addition, no normal control group was included in the present study. Finally, this is a post-hoc analysis of our main study (the CONFIDENCE study) and the sample size calculation was based on the primary outcome of the CONFIDECNE study instead of this post-hoc study. As a result, the possibility that the negative findings in our study could be due to the sample size cannot be ruled out. We intend to address these limitations in a future study.
{kind=link}