4.1 Integrated Care Model Explained
The objective of this study is to build a socio-economic framework of integrated care management of service delivery. Integrated care pathway is designed for chronically ill patients with complex health problems transferring from the hospital to community services and being supervised by their general practitioner.
Health Economics (HE) modelling is mainly used for decision-making purposes and it is an essential part of healthcare planning. A systematic approach to decision making is decision-analytic modelling; economic models usually weight risk, benefits and costs of the options available. The logical mathematical framework of an economic model integrates facts and values and links these data to outcomes that are of interest to health-care decision makers. Economic decision models identify the most cost-effective intervention, the one that produces the greatest health care benefit with resources available [15].
Actual economic evaluation framework and perspective perform mechanisms that influence costs and outcomes and design a study capable of answering the questions: which interventions, for which patients, in which settings, using which resources?
Theories and methods should be explored in order to systematize their inclusion in the economic evaluation of integrated care and service delivery. Donabedian [16] advocated that the quality in healthcare should be evaluated in terms of “structure”, “process” and “outcome”. This approach can be summarised with three questions “who & what resources”, “how” and “with what result”. This service delivery model encompasses several stakeholders: patients, carers, purchasers of healthcare, providers of healthcare and constituent elements. The latter are made up of inpatient and outpatient facilities and staff, which can be referred to as “service line providers”.
This study is going to analyze the structure of Puglia Care chronic care [4][17][18] exploring its technical framework and identifying the functional and clinical roles of its interrelated components, and so providing development of new professional figures [19]. The idea is to set hypotheses to improve the actual model and re-framing it, in order to build an evaluative framework for performance management, decision making and sustainable planning.
After addressing the basic principles and elements of Puglia Care, this study explores two methods for costing the integration of care, those are Service Line Management (SLM) and Time-Driven Activity-Based Costing (TD-ABC). This conceptual framework of the integrated model will aim to assure cost-effectiveness, efficacy and sustainability.
Service Line Management (SLM) is usually applied to improve the management (quality and productivity) of an existing intervention through a bottom-up costing analysis. Operational Research (OR) describes how services are configured and delivered, how resources should be distributed between areas, populations, programmes of care and settings; the location and accessibility of services; the size, composition and skills of the workforce; methods to improve compliance with safety and effectiveness guidelines. SLM is a process for managing the care process and aimed primarily at hospitals. This method can widen its potential opportunities for quality and productivity improvements from overlooking at clinical pathways across care settings, although can face struggles in a period of financial pressure [20].
Time-Driven Activity-Based Costing (TD-ABC) method is a more detailed approach since relies on process mapping techniques to accurately monitor all human and technology resources that contribute to a process of care [21]. It identifies resource utilization at each step of the provider team and can be taken down to individual patient level. This method is used for quality improvement, identifying which step of the process contributes to high costs and which step is delivered in efficient way. It is a technique that improves efficiency as well produces benchmarking across different sites proving the same care objectives and outcomes. TD-ABC is a technique enabling disinvestment of services which could be necessary after changes to the process of care that improve patient outcomes.
4.2 model requirements
Care Puglia utilized real world data from the Assisted Therapeutic Diagnostic Pathway (PDTA) database for their chronic care model. Before-after analysis of Puglia Care model shows a reduction of incidence of unplanned hospitalisation from 12.1 (95% CI, 10.7-13.8) to 10.3 (95% CI, 9.1-11.7) per 100 person/year. The results testify to a significantly lower number (IRR, 0.79; 95% CI, 0.68–0.91), length of hospital stay (IRR, 0.80; 95% CI, 0.76–0.84), and costs related to unplanned hospitalizations (IRR, 0.80; 95% CI, 0.80–0.80) during follow-up in the intervention group [4].
Building up from this promising output, this study is aiming to incorporate in a socio-economic health-integrated care framework a core team performing in a community-based environment. This team represents the “situational awareness” component of the integrated model with specific tasks and roles.
This Situational Awareness Team (SAT) works closely together on patient’s Individual Care Plan (ICP) with the aim of improving clinical and functional patient’s state, minimising symptomatology, preventing disability and sustaining overall quality of life. This Team is going to be responsible of suggesting on investment of community-based resources allowing the patient’s access to health and social services home-based and supervising his/her social isolation. Ultimate outcome should be reducing hospitalisation and delaying institutionalisation.
Functional roles of the team are distinct and, at the same time, coadjutant. The care co-ordinator (professional nurse) works closely to the care regulator (Healthcare-Social Operator - HSO) on case by case, and both report regular follow-up to the GP, functioning as clinical leader. Each Individual Care Plan would fit into a specific health state categorisation (risk stratification) with specific care provision requirement. Mild to moderate cases are dealt by the GP and moderate to severe cases by consultant specialists. The time component in the model is an essential factor in order to monitor service provision and time series analysis of costs and outcomes (Figure 1).
The Individual Care Plan will be part of Health Educational Agenda. This is composed by two parts, patient’s vadevecum (from Latin literal meaning ‘come with me’, concise manual with instructions) and patient’s curriculum (from Latin literal meaning ‘race-course’, course of deeds and experiences through which people become mature), the latter describes patient’s learning process. Patient’s curriculum is a dynamic progress forging life-long learning competency, health literacy and social attitudes. This curriculum would report raised awareness, preventive and positive health seeking behaviour. Three main tasks of care regulator are risk assessment, formation and monitoring/evaluating chronic health state (this is part of the sustainability plan of the model) (Figure 2).
SAT guarantees access to local services network, providing health and social assistance rather than exclusively nursing. So, the socio-economic integrated care model is focused on establishing deeper local authority involvement, improve information sharing, closer working with the voluntary and community sector, independent sector organisations and communities. There is limited evidence of engagement with the voluntary and community sector to date, but this is planning to be the strength of the model. Care coordination and care regulation should be monitored by the SAT, providing patients with self-management strategies, health coaching and social support. Chronic patient is going to feel empowered to understand and manage his/her chronic disease home based with a supported network [2].
There are needs to be addressed and significant barriers to be solved while developing a functioning socio-economic health-integrated model. SAT is expected to smartly fuse different types of information generating a real-time sense-check; a sort of collective intuition on hurdlers and pitfalls which hinder a well-functioning health integrated-system.
Figure 3 describes Socio-Economic Integrated Care Framework using Community-Based Resources (Situational Awareness Team).
This model is going to define the social and economic impact of the community based integrated model (impact assessment). Model design will try to capture common practice within a best & worst scenario. Population will be stratified by mild, moderate and high-risk chronicity, hence indicators along the pathway should describe progress of chronic condition in the pathway undertaken and foreseeable actions. The model can be used to service capacity and quality purposes (health professional workforce capacity and expertise) and cost effectiveness validation of the integrated process.
4.3 model objectives
Three main objectives of the model are management performance, health economics and sustainability plan (Figure 2).
Management Performance – Based on Assisted Diagnostic and Therapeutic Pathway (PDTA)
Care Puglia is currently monitoring pathologies and its current focus is on chronicity. The implementation of Socio-Economic Integrated Care Framework will oversee Care Puglia healthcare management and financial performance.
Healthcare Resource Utilisation at sector level (such as primary, secondary and community care) should be specified, highlighting inefficiencies and adverse events including their costs and how they are reimbursed. The model would be a “real world” experience rather than a “theoretical pathway”. The overall scenario should describe a cross functional team and reproduce overall outcomes at the end of the clinical condition trajectory. Little is known of chronic care management at “community level”, this integrated model can incorporate factors that have an impact on patient’s health state, such as isolation, patient’s network at community level and tertiary sector (Figure 3).
Cost-Effectiveness Analysis – Based on Time-Driven Activity Based Costing
The integrated model should develop both a value proposition and a business case for adoption of a new intervention. This socio-economic model is supportive in designing new intervention and their implementation in clinical practice. Model should specify where in the path the new intervention would fit, based on existing evidence. The intervention could develop a new service or modify an existing one. Assessing the potential cost of the new pathway, identifying resource utilisation of the revised path and QALYs (Quality Adjusted Years Gained) [22]. The methodology of the Cost-Effectiveness plan is going to set performance indicators and create standards for best practice. Socio-economic integrated-care model is going to act as an economic evaluation context that evaluates the economic and effectiveness impact of new interventions on the health system [23].
Stakeholders should define also potential impact of investment and disinvestment in resources at each sector level. Cost analysis of resource utilisation will be based on Time Driven – Activity Based Costing (TD-ABC) [24]. Decision Analysis will explore a potential method to compare complex interventions through Multi-Criteria Decision Analysis (MCDA), involving different stakeholders, considering different healthcare perspectives and scenario analyses. Decision makers of local authorities would benefit from this advanced method, which will allow to incorporate all relevant categories of outcomes and costs [25]
Sustainability Plan – Based on Indicators Matrix
This model describes chronic conditions which, by nature, are degenerative diseases.
SAT represents a determinant of sustainability enhancing an ecological public health education plan at community level, incorporating environmental and climate mediated health risks.
The newly emerging care-regulator role will adopt a holistic approach and action agenda towards sustainable ways of living at home, aiming toward sustainable health development. Care regulator would enhance and foster the desirable health seeking behaviour by promoting a greater sense of health awareness and joint responsibility. Hence, he would represent a “health-educator” raising patients’ awareness, influencing their attitudes and improving overall health. Health educational agenda will include all healthy activities which empower patients acquiring skills, attitudes and essential values for personal development.
The main sustainability outcome of this framework is delaying the progressive health state degeneration. Socio-economic Integrated Care Model will design sustainability scenarios reflecting perspectives of multiple stakeholders and capturing variables at multiple levels of health delivery.
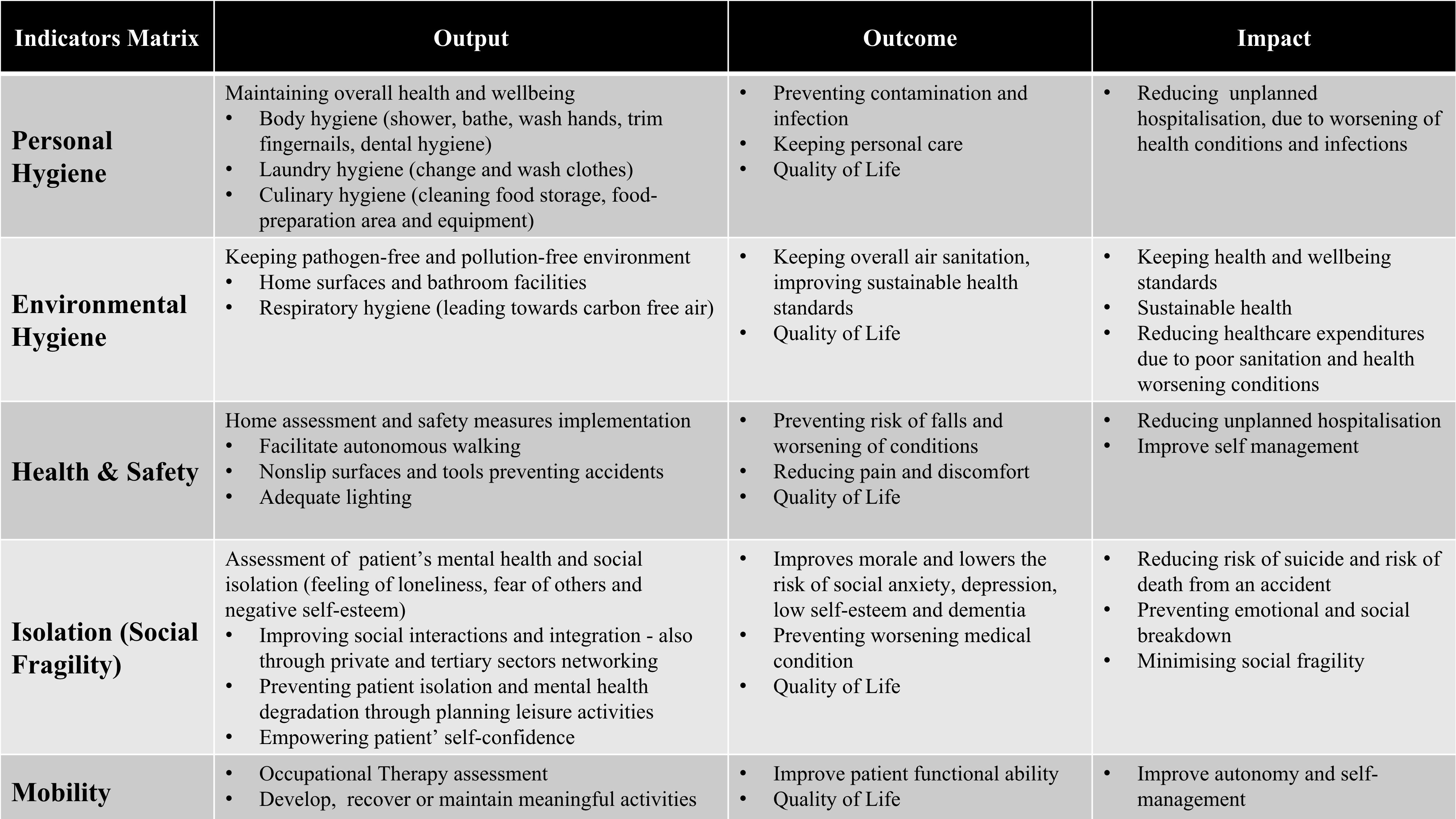
Timeframe will be reviewed collecting indicators values at multiple time points. Indicators matrix (Table 1) will monitor and evaluate the sustainability process. Short term review will indicate an organisational control, medium-long term will define behavioural change and describe impact.
Sustainability plan is based on five indicators, measured at short, medium and long term, personal hygiene, environmental hygiene, house health & safety, isolation (social fragility), and mobility (occupational therapy) (see table 1).
A Vector Autoregression (VAR) model will be used to measures a multivariate time series especially for describing the dynamic behavior on the use of the selected indicators. In addition to data description and forecasting, the VAR model, will be used for structural inference and policy analysis.
4.4 implementation of integrated model
The integrated model, by its ability to converge to common goals, create flexible functioning toward a mission led perspective. Healthcare-Social Operator (HSO) is a qualified professional figure with health and social qualifications (Puglia RR n28, 18th December 2007). Currently the HSO acts as a hybrid figure supporting nursing and social care. Its peculiar role fits perfectly into the current healthcare domiciliary setting (see Appendix B). Puglia Region is currently forming a constant number of HSO every year (n=127) with a cost of € 8.300 per HSO formed per yearly.
This socio-economic framework requires an upgraded HSO figure to care-regulator role able to monitor a patient’s health education agenda and individual care plan. We are going to set focus group discussions to discuss the new care-regulator role its professional functionality and formation required to explicate his functions.
Structure of the pilot model structure can be built from domain knowledge, as described by the healthcare experts, while the detailed parameter must be extracted by geo-statistical estimation techniques and validated using the available data (e.g. PDTA). The analysis is going to follow the patient’s clinical pathway and his transition into different stages of illness.
Simulated model analysis is going to be implemented as a feasibility work on the territory reporting time driven integrated care activities as in figure 1. This implementation plan is going to be extended to six local health authority (Ba, Br, Bt, Fg, Le and Ta) as described in Appendix C covering Puglia Region. SAT implementation along PDTA is going to be a dynamic process supporting decision making.
{kind=link}