Study population
Hundred-and-twelve rTOF patients, in whom LAS was feasible and were in sinus rhythm, were included in the final analysis (age 33±10 years old, 68[61%] male). The overall feasibility of the LAS measurements was 87.4%. Twenty-three patients (15.2%) were excluded due to poor image quality or poor tracking, while 22 patients (14.6%) were excluded due to a baseline rhythm other than sinus.
Baseline characteristics of the study patients are summarized in Table 1. Patients in the lower LAS-r tertiles were significantly older(36±11 vs 31±9 vs 32±9y, p=0.034), had a larger initial repair age (4[2-9] vs 2[1-5] vs 2[1-5]y, p=0.036), and had greater proportion of Waterston shunt as the initial repair(21% vs 5% vs 6%, p=0.030). Cardiac medication use was also significantly higher in the lower LAS-r tertiles(37% vs 3% vs 3%, p<0.001).
Distribution of baseline electrocardiographic, echocardiographic and laboratory parameters in the study group is demonstrated in Table 2. QRS duration was significantly higher in the lowest tertile group(155±29 vs 127±32 vs 133±28ms,p<0.001). LVEF (52±8 vs 54±5 vs 56±5%,p=0.034), and E’ amplitude was lower in lower tertiles(8±3 vs 9±3 vs 9±2cm/s,p=0.042).
Left atrial volume and function
Distribution of LA, LV and RV STE parameters among LAS-r tertiles is demonstrated in Table 4. All the LAS and LASR values were decreased in lower tertiles. LV-GLS and LV-Sre were significantly lower in lower tertiles, however RV-FWLS didn’t differ significantly(LV-GLS:-16.8±3.5 vs -18.3±2.8 vs -18.4±2.8%, p=0.005;LV-SRe: 0.7±0.2 vs 0.8±0.2 vs 0.8±0.2,p=0.009;RV-FWLS:-14.9±4.3 vs -16.5±3.4 vs -16.5±3.3,p=0.14).
Follow-up and assessment of endpoints
Overview of the events observed during follow-up are summarized in Supplemental table-2. Median duration of follow-up was 8.6[4.2-9.7] years in the study group. During follow-up, 98 events occurred. 33 patients underwent surgical or transcatheter intervention. 18 patients had an arrhythmia episode, and 8 patients had a heart failure episode requiring treatment. 37 patients were hospitalized during follow-up. There were two deaths: 1 due to viral pneumonia, the other due to sudden cardiac death. The primary composite endpoint of any event was observed in 48 patients (mean event-free survival time: 7.2[6.6-7.9] years), while the secondary composite endpoint of death, heart failure or arrhythmia was observed in 22 patients (mean event-free survival time: 8.7[8.1-9.2] years).
Baseline clinical and echocardiographic predictors of prognosis
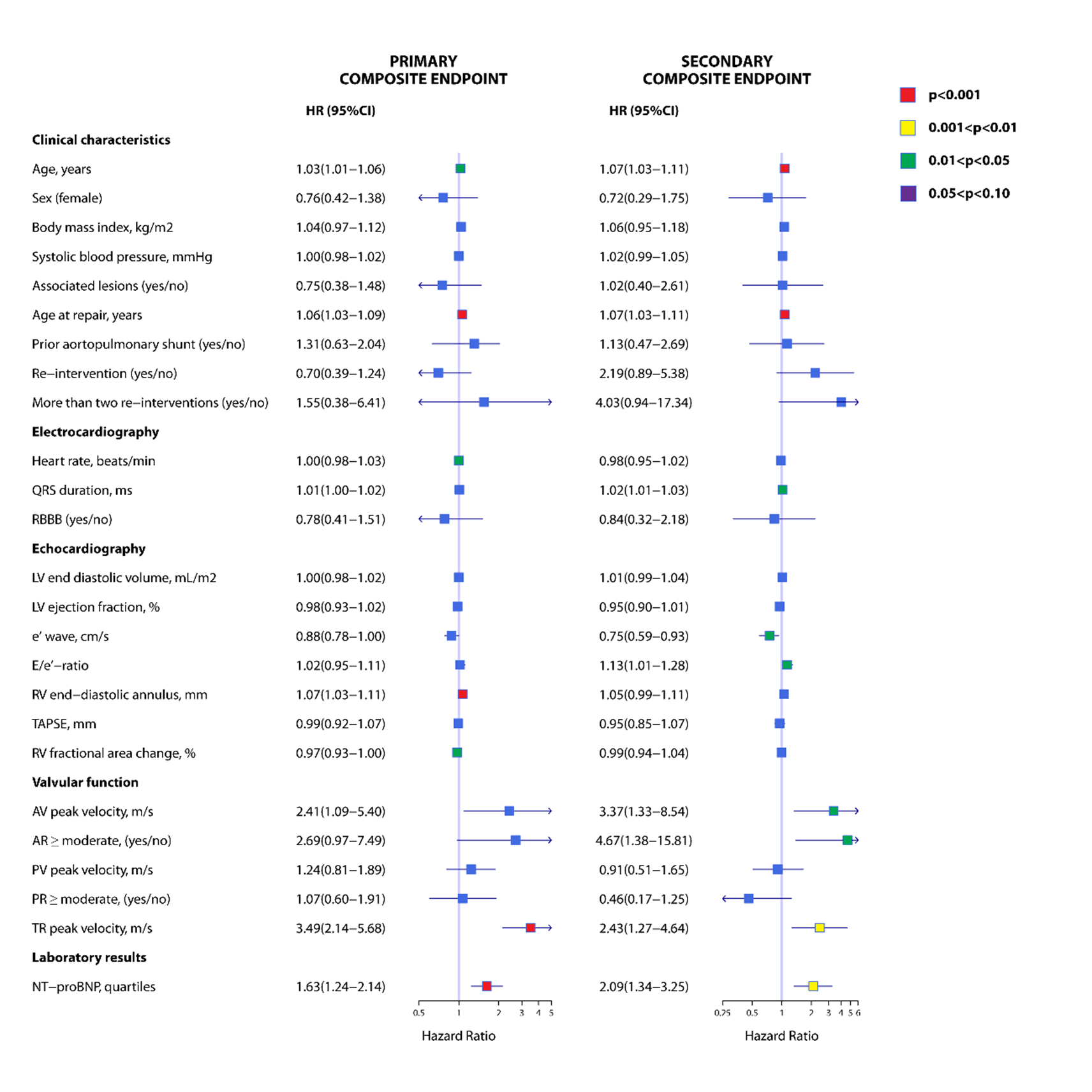
Baseline characteristics associated with composite endpoints are shown in Supplemental Figure 1. In univariable Cox regression, age, age at repair, QRS duration, e’ wave, AV peak velocity, AR of more than moderate degree, TR peak velocity and increasing tertile of NT-proBNP were associated with primary and secondary endpoints. RV end-diastolic annulus diameter and TR of more than moderate degree was associated with primary, while E/e’ ratio was associated with secondary composite endpoints.
Association of LA speckle tracking parameters with prognosis
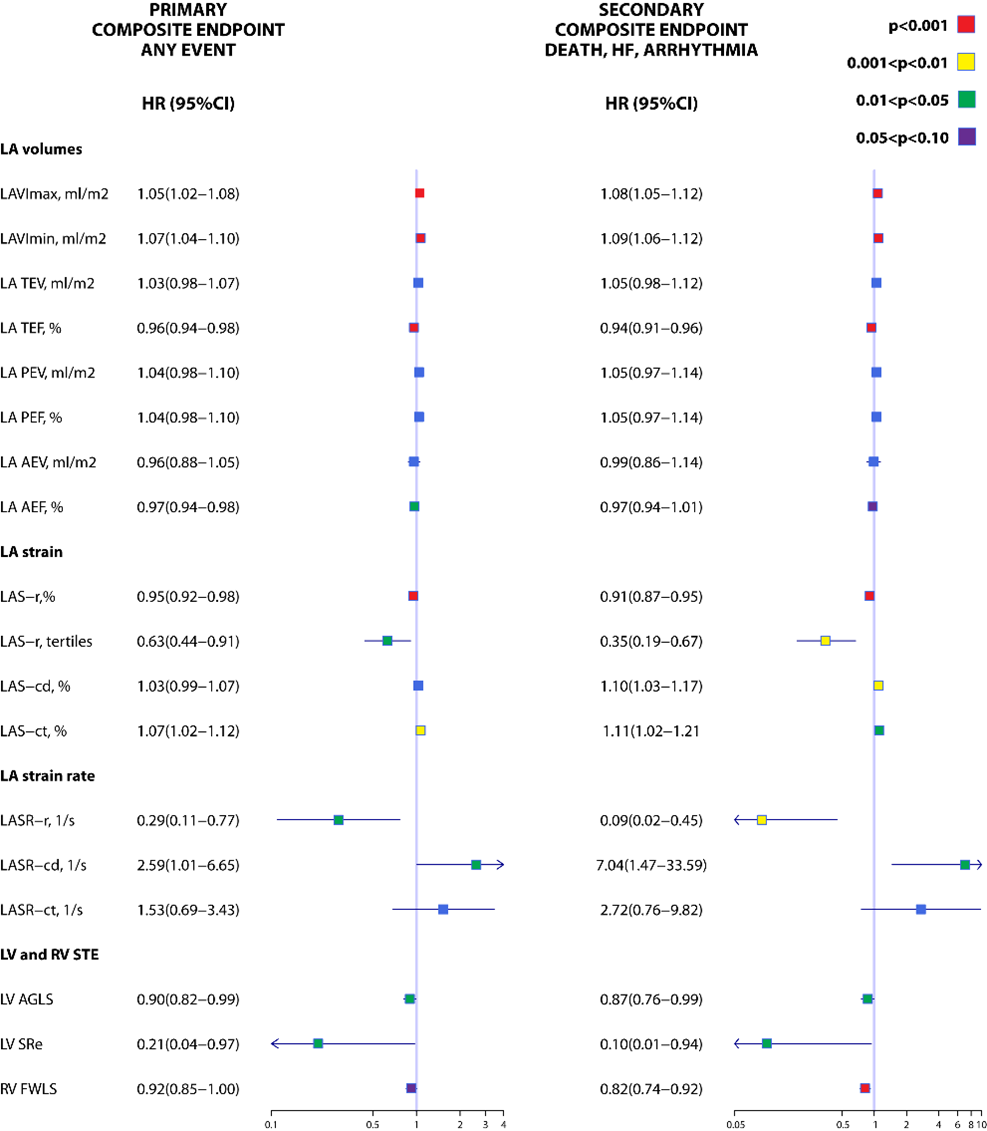
Univariable analysis showing association of speckle tracking parameters with prognosis is shown in Supplemental Figure 2. In univariable cox regression, increased LAS-r was associated with primary and secondary composite endpoints. In Kaplan-Meier analysis, decreasing tertile of LAS-r was associated with decreased event free survival from primary and secondary composite endpoints (mean survival=5.9[4.7-7.1] vs 7.8[6.8-8.8] vs 7.9[6.8-9]years,p=0.020 for primary; 7.2[6-8.5] vs 9[8.3-9.7] vs 9.7[9.1-10.2]years,p=0.002 for secondary composite endpoints) (Figure 1A and 1B, respectively).
When adjusted by initial repair age and NT-proBNP quartiles, increased LAS-r was associated with significantly decreased occurrence of any events(HR=0.97,CI:0.93-0.99,p=0.037]). When adjusted by baseline echocardiographic parameters e’ wave, RVEDD, TRV, TR of at least moderate degree, AV peak velocity, and AR of at least moderate degree, and increasing LAS-r was associated with decreasing occurrence of primary composite endpoint(HR=0.95,CI:0.91-0.99,p=0.016). In a third model, when adjusted by LAVImax, increased LAS-r was associated with decreased occurrence of primary composite endpoint(HR=0.96,CI:0.03-0.99,p=0.01). LAS-r was significantly associated with primary endpoint when also adjusted by LV-GLS(0.95,95%CI:0.92-0.98,p=0.002) or RV-FWLS(0.96,95%CI:0.93-0.99,p=0.04).
{kind=link}
{kind=link}