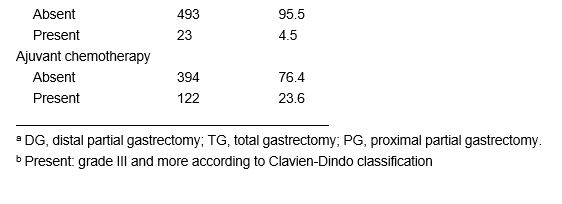
In this study, we first demonstrated that 13.8% of patients who underwent gastrectomy for GC experienced readmission within one year. Choe et al. reported that 11.7% of patients were readmitted within one year after gastrectomy[13]. Kim et al. reported that the 5 year-readmission rate was 13.0% in patients who underwent radical subtotal gastrectomy for early GC[9]. They also reported that approximately 80% of patients were readmitted within one year, indicating that the one-year readmission rate was approximately 10%. The one-year readmission rate in this study was slightly higher than their results, which might be due to the inclusion of advanced GC in our study and the difference in health insurance systems.
Because gastrectomy reduces the volume of the stomach, many patients who have undergone gastrectomy for GC experience nutritional difficulty due to insufficient food intake after surgery. Food intake gradually increases in most patients as the number of postoperative days increases. However, food intake sometimes decreases again in some patients after they leave the hospital because it is often difficult to prepare suitable food at home for post-gastrectomy patients. Such patients are likely to be rehospitalized for nutritional support. Patients who undergo gastrectomy for GC are expected to be at high risk of readmission due to poor food intake when compared with patients who undergo surgeries other than gastrectomy. In fact, nutritional difficulty after gastrectomy was the second leading cause of readmission in patients who underwent gastrectomy for GC in this study. This study revealed that the interval from primary discharge to first readmission due to nutritional difficulty was significantly shorter than that due to other causes. In fact, 50% of patients with readmission within one year experienced 30-day readmission in this study. Therefore, the short interval from primary discharge to first readmission was the unique characteristic of readmission due to nutritional difficulty compared with readmission due to other causes.
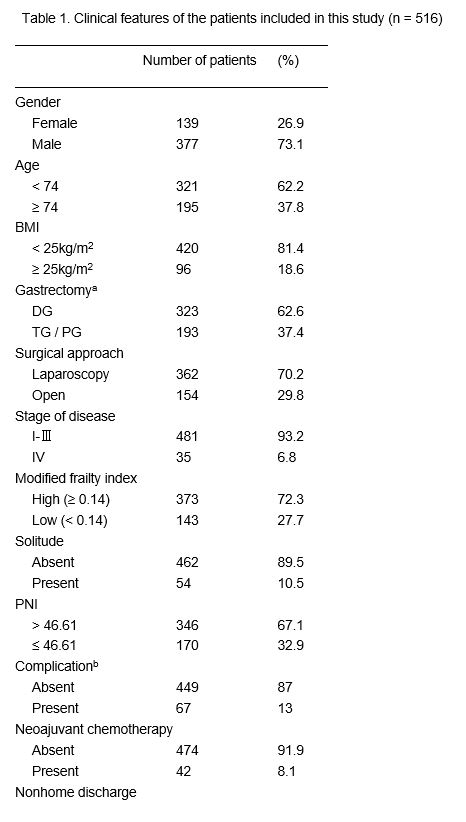
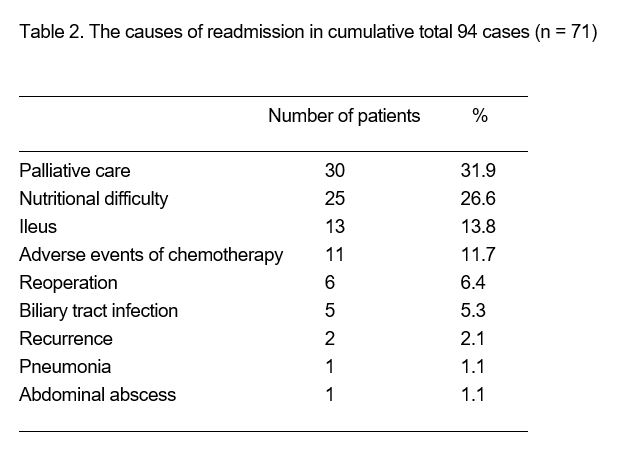
It is important to note that readmission due to nutritional difficulty could be avoidable. Baker et al. have suggested that home enteral nutrition for 6 weeks through a feeding jejunostomy tube did not affect oral intake of a regular diet and improved postoperative nutrition following TG[6]. Recently, oral nutritional supplements (ONS) have been of great interest as perioperative nutritional interventions in patients with GC who underwent gastrectomy. Kimura et al. demonstrated that administration of 300 kcal/day of ONS for 6 to 8 weeks in the early post-gastrectomy period reduced body weight loss not only at 6 to 8 weeks postoperatively but also at 1 year in patients who underwent TG[7]. Therefore, nutritional support might be useful in preventing readmission due to nutritional difficulty. However, it is not practical to provide intensive nutritional support for all patients who undergo gastrectomy for GC. Therefore, it is indispensable to predict patients who are at high risk of readmission due to nutritional difficulty and provide intensive nutritional support for those patients. In this study, we identified that the type of gastrectomy and the mFI were independent predictive indicators for readmission due to nutritional difficulty. With regard to the type of gastrectomy, total gastrectomy and proximal gastrectomy were risk factors for readmission due to nutritional difficulty. According to the Post Gastrectomy Syndrome Assessment Study, one-year body weight reduction rates after gastrectomy for GC were 13.8 %, 10.9 %, 7.9 % and 8.9 % in TG, PG, DG with Billroth-I reconstruction, and DG with Roux-en-Y reconstruction, respectively, indicating that higher body weight reduction rates were observed more frequently in patients with ether TG or PG than in those with DG[14, 15]. Therefore, patients who underwent ether TG or PG are more likely to have nutritional difficulty after surgery than those who undergo DG. Furukawa et al. recently reported that subtotal gastrectomy with a very small remnant stomach had more favorable short-term outcomes and nutritional status than total and proximal gastrectomy[16]. Even though the remnant stomach is very small, it seems to be useful in maintaining ghrelin secretion and reducing gastro-esophageal reflux through preservation of the gastric cardia, which contributes to a favorable postoperative nutritional status. Therefore, it might be possible to reduce readmission due to nutritional difficulty through the improvement of surgery.
Frailty is a syndrome characterized by decreased physiological reserve. It has been reported to be associated with an increased risk of adverse outcomes in patients who undergo surgery[17–20]. A standardized, quantifiable assessment of frailty may enable surgeons to evaluate patients’ risk of adverse outcomes after surgery. Therefore, the development of a useful and less complex tool to evaluate frailty is indispensable to improve patient outcomes. The modified frailty index (mFI) is one such tool based on the assessment of 11 physiological deficits collected by the American College of Surgeons National Surgical Quality Improvement Program (NSQIP)[11]. These 11 items are easily identifiable during patient encounters and are defined as the proportion of potential deficits that are present in an individual to the 11 potential deficits that were evaluated. The mFI has been found to be predictive for postoperative short-term outcomes in several surgical populations, including patients undergoing abdominal, vascular, and head and neck surgery[21–24]. However, the correlation between mFI and readmission due to nutritional difficulty has not been well determined so far. In this regard, Choe et al. reported that preoperative assessment of frailty could predict readmission within one year of discharge after gastrectomy[13]. In their study, frailty was assessed using the Study of Osteoporotic Fractures frailty index. Furthermore, all causes associated with one-year readmission were included in their study. On the other hand, we used mFI to evaluate frailty and found a close correlation between mFI and one-year readmission due to nutritional difficulty. Our study clearly demonstrated that frail GC patients were at high risk of readmission due to nutritional difficulty. This indicates the possibility that frail GC patients find it more difficult to adjust to the post-gastrectomy status than non-frail GC patients. To the best of our knowledge, this is the first study to demonstrate the close correlation between mFI and one-year readmission due to nutritional difficulty.
Our study demonstrated that the combination of mFI and the type of gastrectomy was more useful in predicting readmission due to nutritional difficulty than single use of those indicators. Because readmission rate due to nutritional difficulty was high in patients who underwent either TG or PG with high mFI, intensive follow-up and nutritional support should be performed in such patients to reduce readmission due to nutritional difficulty.
The present study had some limitations. First, its retrospective design was associated with some bias. Second, only a small number of patients were included, and a larger trial is required to confirm our results. Third, all patients included in this study were Japanese. Because insurance systems are different for each country, the indications for readmission might also be different for each country; this is likely to affect the predictive factors for readmission.
In conclusion, we demonstrated that the type of gastrectomy and the mFI were predictive indicators for readmission due to nutritional difficulty in patients who underwent gastrectomy for GC. Because the readmission rate due to nutritional difficulty was high in patients who underwent either TG or PG with a high mFI, intensive follow-up and nutritional support should be provided in such patients to reduce readmission due to nutritional difficulty, to improve patients’ QOL and prognosis, and to reduce additional medical costs.
{kind=link}
{kind=link}
{kind=link}
{kind=link}