Forced expiration against an airway obstruction was originally presented by Antonio Maria Valsalva (1666 – 1723) as a method to inflate the Eustachain tubes [1, 5, 6]. The VM, which is now used as a procedure to investigate the function of autonomic system, can be divided into four physiological phases [4, 7]. Physiological variations in phase 2 and phase 4 of the VM are accompanied by the change of both autonomic excitability and hemodynamics. The increased intrathoracic pressure causes an obstruction of venous reflux in phase 2, stimulating the sympathetic increased excitability. And in phase 4, parasympathetic activity is increased, resulting in relatively quick slowing down of the heart. Therefore, baseline, phase 2 and phase 4 were selected in this study, to detect the dual effect of the VM on parameters in individuals at different phases [5-7, 10]. Compared with baseline (83 ± 11.73 bpm), we found a significantly increased HR in phase 2 (92 ± 14.28 bpm, p < 0.001) and a significantly decreased HR in phase 4 (80 ± 10.15 bpm, p = 0.030). Also, HR in phase 4 is significantly lower than it in phase 2 (p < 0.001). These results were consistent in numerous previous studies [5-7]. HRV is a simple, noninvasive method to evaluate the autonomic nervous system regulation and has been used in a variety of clinical situations. It is the variation in the time interval between each heartbeat which is recorded as R – R intervals [15]. Traditional HRV assessment methods include time domain, frequency domain and nonlinear analysis. LF (0.04 – 0.15 Hz) and HF (0.15 – 0.4 Hz) are two of basic components of frequency domains. A higher HF specifically shows that parasympathetic activation is increased, while the attribution of LF is widely debated and generally considered to be the combined sympathetic and parasympathetic influence [16, 17]. In recent studies, the LF/HF ratio is used as a measure of the global sympatho-vagal balance and can be used to indicate the amount of sympatho-vagal modulation of the instantaneous heart rate. An increasing LF/HF represents that sympathetic activation is predominant [18]. Compared to baseline, we found a significantly LF/HF ratio in phase 2(1.44 ± 1.64 vs. 7.48 ± 11.61, p = 0.024) that reflected an increased sympathetic activity, and a significantly increased HF indices in phase 4 (2546.08 ± 1837.11 vs. 1206.04 ± 1206.07 mm2, p = 0.04) reflecting a hyperfunction of parasympathetic nerve.
The elevation of IOP in healthy individuals during the continued strain of the VM has been reported in numerous studies [4, 9, 10, 19]. It has been speculated that IOP elevation in phase 2 of the VM is mainly caused by raised episcleral pressure reducing aqueous outflow. The anterior engorged choroidal vessels may make a small increase of the total ocular volume resulting in an elevation of IOP, because the wall of the eye has certain rigidity [20]. We also observed that, relative to baseline, phase 2 of the VM in young healthy adults led to an elevation in IOP (15.1 ± 2.7 vs. 18.8 ± 3.5 mmHg, p < 0.001). A study by Li et al. showed that the anterior choroid and the ciliary body but not posterior choroid were thickened during forced exhalation against a closed airway in phase 2 [21]. Significantly decreased AOD500, ARA750, TIA500 and TISA500 during the VM may be another reason for elevated IOP, because a narrowed anterior chamber could lead to higher outflow resistance of aqueous humor [22]. In our study, IOP returned to baseline in phase 4 rapidly, since this phase is the normal process of physiological indexes with the resistance to blood flowing disappear. In addition, autonomic activity frequently influences IOP. Increased HR and LF/HF ratio found in phase 2 implied a sympathetic activation, while significantly increased HF and remarkably decreased HR in phase 4 showed a parasympathetic excitation. These results contrast with previous studies that suggested an active sympathetic nervous system may lead to a decrease in IOP, while overactivation of parasympathetic nerve can produce an elevation of IOP [13, 23, 24]. Therefore, we speculate that the IOP fluctuation arise from the changes of blood flow and ocular anatomy may counteracted and reversed the influences of autonomic activity.
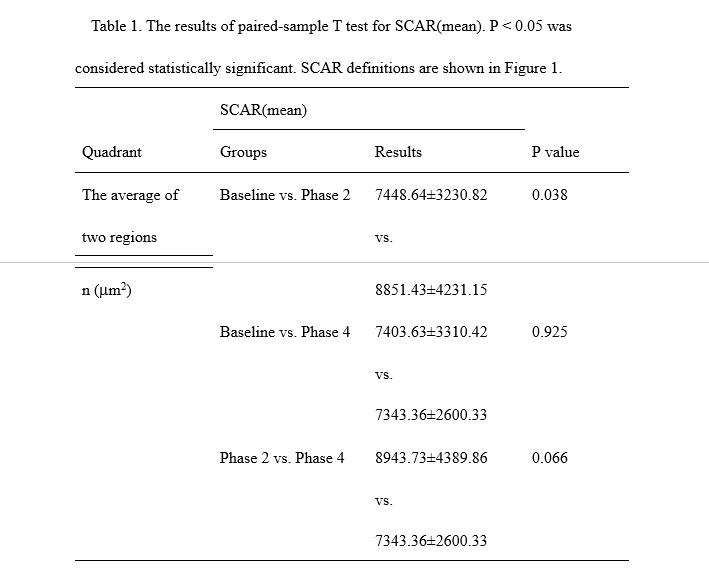
SC is the vein at the chamber angle, which is first discovered by Friedrich Schlemm in 1830, that collects aqueous humor from anterior chamber and delivers it into the bloodstream [25]. In previous study, Chen et al. found that the collapse may be one of the reason of the IOP peak after the water-drinking test [14]. And numerous studies have reported that an IOP of 30 to 50 mmHg can make trabecular sheets distended into SC and reduce the SC lumen [26, 27]. However, in this study, the increase in SCAR from baseline to phase 2 (7448.64±3230.82 vs. 8851.43±4231.15 μm2, p = 0.038) , while IOP is significantly increased, is less easily explained. The SC might have autonomic regulation functions [13, 28, 29]. Therefore, the expansion and collapse may not be completely dependent on the IOP. The expansion of SC is possible to be caused by sympathetic nerve stimulation in phase 2 of the VM. Although the average of SCAR in phase 4 become lesser than it in baseline and phase2, there was no significant differences. It has been indicated that activation of parasympathetic nerves might be involved in the collapse of SC in previous study, and parasympathetic system was found excited in phase 4 in this study [13, 14]. But there were only 13 individuals showed a smaller SCAR in phase 4 than SCAR in baseline. We speculated that this result might relates to individual diversities in the rate of autonomic regulation, because only 15s after subjects recovered normal breath was took into account and this time may be too short for some individuals to finish the regulation.
According to previous studies, elevation and fluctuation of IOP are associated with the development and progression of glaucoma [30]. In this study, we found that breath holding in phase 2 has an additive effect on IOP, which is consistent with previous studies. It has been reported that the VM can make the IOP of patients higher than normal, in whom the IOP is near to the 20mmHg border [31]. MOPP represents the gradient of efficient perfusion for all intraocular structures, including the optic nerve head and the retina.[32] The remarkably elevated IOP we found in phase 2 resulted in a reduction in MOPP (46.06 ± 6.61 vs. 41.23 ± 7.49 mmHg, p = 0.002). Although the MOPP started raising in phase 4, a short time is difficult to recovery, as the MOPP in phase 4 was still significantly lower than it in baseline (46.06 ± 6.61 vs.44.53 ± 6.15 mmHg, p = 0.017). There was an associated possibility of mechanical and ischemic damage to the optic nerve head, leading to glaucoma process [30, 32].
Pupil diameter, which is controlled by the sphincter pupillae and the dilator pupillae, is the reflection of iris size. The sphincter pupillae is primarily controlled by the parasympathetic nervous system, and the dilator pupilae is primarily controlled by sympathetic nervous system [33]. The pupil diameter (PD) were found to be dilated in phase 2 (4.23 ± 0.82 vs. 4.74 ± 0.74 mm, p<0.001), and the PD in phase 4 (4.47 ± 0.73 mm) declined markedly in comparison with the pupil diameter in phase 2 (p = 0.001), and meanwhile still obviously greater than it in baseline (p<0.001). It indicates that the activation of sympathetic nervous system caused by the VM was sufficient to invoke pupil dilation, and it took some time to be back to normal. A prolonged pupil dilation might be a precipitating risk factor of PACG patients in routine life [34, 35].
The VM is very common in our daily life, and is done automatically and briefly, in vomiting and coughing and sneezing, and for longer periods in bodily functions like parturition and defecation; more deliberately, in heavy lifting; in various sports; in the blowing of wind instruments, and even in singing and laughing [1]. Changes caused by the VM in healthy young individuals may carry no clinical significance, but for patients with high risk factors of glaucoma, we suggest that it may be good to avoid repeating VMs in daily life.
This study had limitations. First, only 15 seconds after subjects recovered normal breath were observed in this study. It may be too short for physiological indicators of all individuals to return normal. Next, it is unclear whether similar effects of VMs would be observed in elderly subjects or patients with glaucoma, for all of our individuals were young and healthy. Lastly, the thickness of anterior choroid in AS-OCT images we gained in this study. It is necessary to acquire a more detailed data set in a future study.
In conclusion, the expansion and collapse of SC in different phases of the VM may cause by changes of autonomic nervous system activity, while its influence on IOP could be counteracted even reversed by the changes of blood flow and ocular anatomy.
{kind=link}