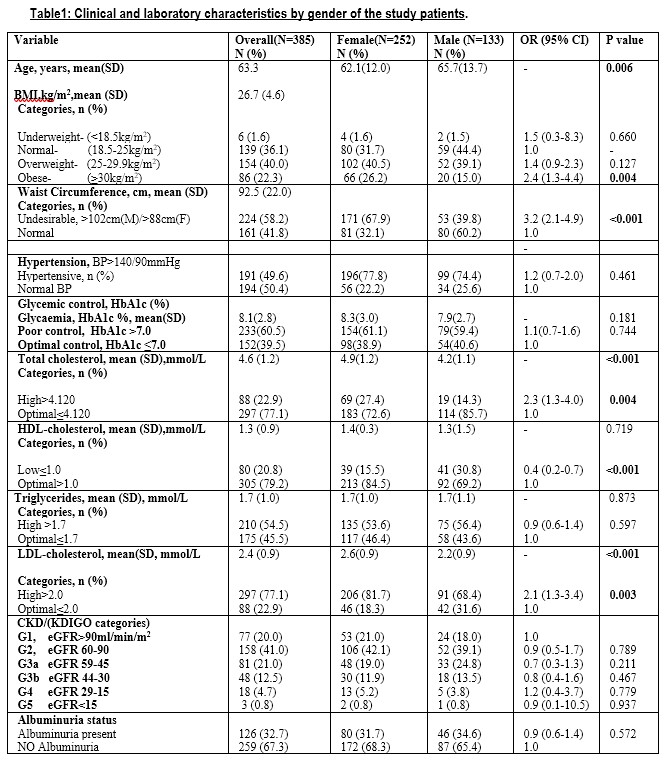
This adult population of 30yrs and above, with type 2 diabetes had a prevalence of 39.0% (95%CI, 34.3–44.2) with chronic kidney disease (CKD) stages 3 to 5 byeGFR (<60 ml/min/1.73 m2) and 32.7% (95%CI, 32.7–37.4) had albuminuria.Focusing on each CKD-stage, 33.5% were in stage–3, 4.7% in stage–4 and 0.8% in stage–5 in this study. The occurrence of CKD was previously unknown to both the patients and healthcare providers. These advanced stages of CKD are quite often asymptomatic, so patients are not prompted to seek care early. Therefore, it was not surprising that these CKD-stages were not previously recognized.
The policy of cost-sharing in public health facilities may have limited access to both clinical care and laboratory diagnostic services of the patients who could not afford them. This study excluded any patients who had recently been discharged from hospital; therefore the prevalence reported is certainly an underestimate.
The meta-analysis of studies on diabetes kidney disease in sub-Saharan Africa by Noubiap JJ et al(14) gave a summary on methods used and characteristics of the patients involved in those studies, mentioning some shortcomings that limited adequate comparability. Indeed several of those studies analyzed patients with type 1 and 2 diabetes, conditions with fairly divergent time paths towards evolution of kidney disease, even when risk factors may be common.
In this study, we discuss the prevalence CKD stages 3 to 5 in context of its magnitude, clinical significance, opportunities of case-finding and implication to care needs.
Several studies conducted to determine the prevalence of CKD stages 3 to 5 and/or albuminuria in patients with type 2 diabetes in sub-Saharan Africa have exhibited a wide range of figures. Our own previous study on patients with type 2 diabetes for less than 2 years, relatively younger, in a tertiary hospital, found 26% of them had albuminuria.(15) Ngassa et al, in S. Africa found 33.6% of their patients had proteinuria and 17.3% had CKD of stages 3, 4 and 5 (eGFR<60 ml/minute/1.73m2), but these were aggregated for both type 1 and 2 diabetes.(16) The prevalence of CKD in patients with type 2 diabetes was 41.1% in a Nigerian study.(17)Advanced CKD, of eGFR<60 ml/min/1.73 m2, was found in 18.2% and 23.8% of subjects with diabetes using the MDRD and Cockcroft-Gault (C-G) equations respectively, in an Ethiopian study,(18) demonstrating that the equation used to calculate eGFR may also explain variations in prevalence. Two studies on patients with type 1 and type 2 diabetes were conducted in two different places in Tanzania. Janmohamed et al, found 79.9% had albuminuria and 83.7% had CKD (eGFR<60 ml/minute/1.73m2),(19) while Lutale et al, found 17% had albuminuria and 22% had CKD stages 3 to 5.(20) Their methods of determining proteinuria and target populations varied in ages, duration of diabetes and other characteristics. The prevalence of CKD in studies in sub-Saharan Africa is relatively high, in spite of the differences in patient characteristics within diabetes and the methods used. However, CKD and albuminuria still exhibit common determinants of aging, hypertension, poor glycaemic control and socio-economic challenges where they were evaluated. This study did not show glycaemic control as a significant predictor of chronic kidney disease.
Prevalence of advanced CKD, stages 3–5 in Europe is low, 1.0 - 5.6 %, (21) higher in the USA, at 21.4 %,(22) probably due to heterogeneous populations, but still lower than what is found in the developing world as already described. The studies in Europe and USA also reported very low conversion rates of CKD stage 3–5 to end-stage renal disease (ESRD), that is, incidence of ESRD as a percentage of prevalence of CKD stages. However, CKD stages 3 to 5, in clinical terms, are significant inasmuch as they may progress to ESRD by 25 to 45-fold and constitute a large pool of patients at higher risk of cardiovascular disease and events.(23, 24)Resources invested in healthcare, access to care, quality of care and probably, the support to individual self-care (interacting with individual risks like genetics) are the most likely explanatory factors for the differences that we see. Sub-Saharan Africa has lower investment in health, number of care centers and access to care (and inadequate risk factor control) than the developed world.
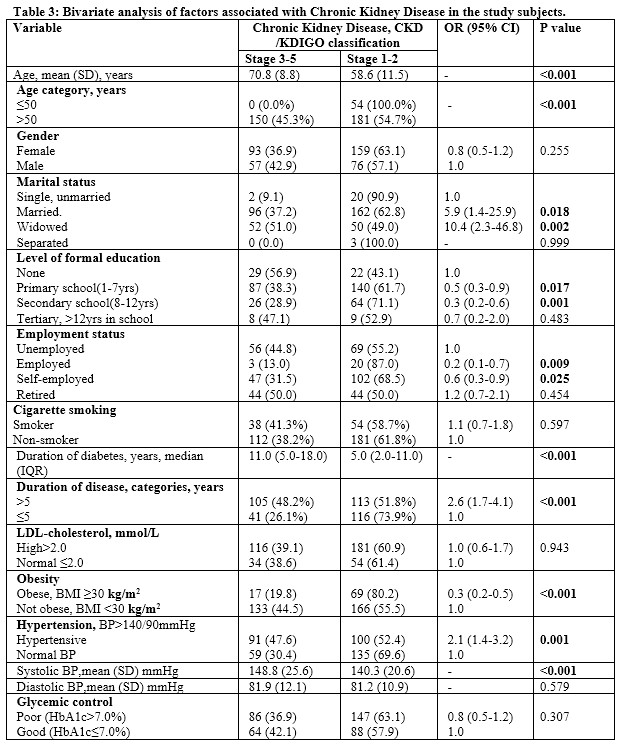
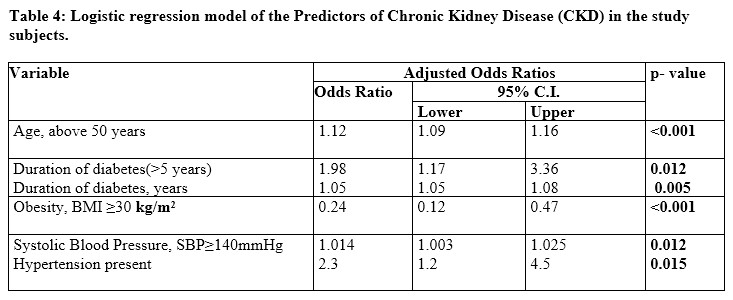
Our study showed that age above 50 years, (and aging per se), was associated with having CKD/KDIGO stages 3 to 5. In addition, living with diabetes for 5 years and more, increased the odds of having advanced CKD stages. Similarly, other studies (recognized and) demonstrated that aging is associated with deteriorating kidney function (25, 26), and long duration of diabetes compounds it.(27) These parameters are easily determined in clinics and should assist in stratifying our patients into risk categories during routine follow-up for enhanced attention, especially in patients with other risk factors like hypertension, chronic poor glycaemic control and cigarette-smoking.
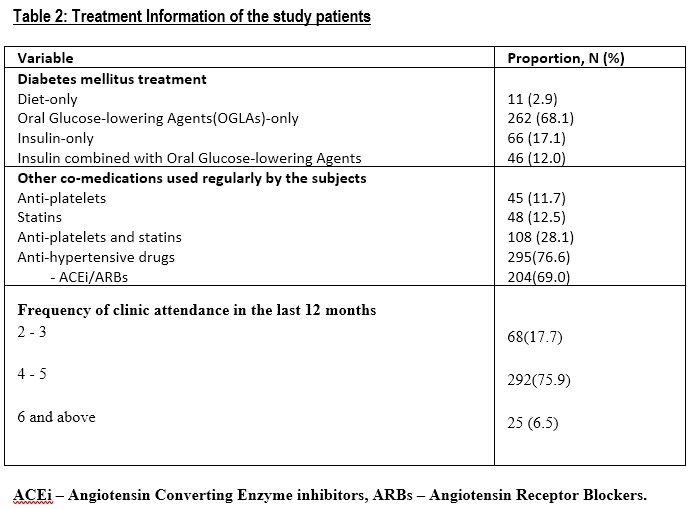
Hypertension, a modifiable risk factor increased by 3-fold, the odds of having advanced CKD stages in this study. Hypertension causes chronic kidney disease in type 2 diabetes (28, 29, 30, 31, 32) and other cardiovascular events like heart failure (33)and stroke (34, 35)but controlling hypertension in such subjects with normal kidney function mitigates the potential for developing CKD. (36, 37) Conversely, poor or insufficient management of hypertension initiates CKD (and a factor of progression of CKD to more advanced stages). Studies have shown use of ACEi’s/ARB’s mitigates renal disease progression. (38, 39, 40, 41) Our study registered 69.0% users of ACEi/ARB agents; however we did not determine duration of use, doses nor the adherence patterns. Just below a quarter of our study patients with hypertension, at the time of enrolment, had optimal control of the high blood pressure. We have previously documented similar modest proportion of patients with hypertension on type 2 diabetes who achieved optimal Blood Pressure control while on treatment.(42) Another study elsewhere in sub-Saharan Africa (43)also reported similar small proportions.
“Usual” care is not as effective as “intensive” care of CKD in retarding progression to advanced disease.(44) We observed sub-optimal control of risk factors in a large proportion of patients, in spite of four and more clinic visits by over 80% of our patients for routine follow-up in the previous 12 months. Specifically, all these patients with CKD were only detected at the time of the study, which suggests that the level of clinical care in this clinic did not have sufficient capacity to detect complications or monitor risk factor control.
REGARDS study demonstrated that socio-economic status (SES) determines access to care and treatment. Modest SES is associated with CKD and patients with individual SES challenges, but not the community one came from, were worse off.(45)Socio-economic challenges abound in Kenya, both in individuals and communities, even amongst our study patients, sufficient to limit the ability of individuals with type 2 diabetes to access and afford quality care for successful secondary prevention of complications.
Obesity of BMI≥30kg/m2 and employment reduced the odds of having advanced CKD stages, the obesity was probably acting as a marker of better socio-economic status in those individuals. Obesity exhibited mitigating effects in its association with CKD and cardiovascular morbidity (and mortality) in an Iranian study.(46)However, obesity is generally associated with chronic kidney disease. (47)
Most of our patients were on oral glucose-lowering agents, 67.8% used sulphonylureas, 78.2% used Metformin and 29.1% were on Insulin–based combinations achieving a mean HbA1c of 8.2(2.1) %. Metformin is central in treatment of type 2 diabetes, not just for lowering hyperglycaemia but also for other non-glycaemic cardiovascular benefits, though its side-effects are aggravated in kidney dysfunction. To derive its benefits and limit its toxicity, use of metformin therefore requires knowledge of eGFR to titrate its dose.(48, 49) Sulphonylureas also can potentially increase risk of clinical hypoglycemia, (50)that would be more frequent in advanced stages of CKD.(51)Our patients were on sulphonylureas and metformin yet their diminished kidney function of CKD was unknown, putting their safety at risk. Similarly, use of other medications like non-steroidal anti-inflammatory drugs (NSAID’s) analgesia,with nephrotoxic potential,(52) may cause further deterioration of CKD stages, thus can be avoided or be used with caution. Screening for presence of CKD is therefore very important for patient safety as well.
From this study we infer that diabetes care in the clinic was neither sufficient to achieve and monitor optimal control of the modifiable risk factors nor able to detect complications in the patients. These findings suggest that patients, with type 2 diabetes for 5-years and more, aged 50 years and above, have hypertension, are cigarette-smokers and of modest socio-economic capacity should be screened for CKD. Many patients with type 2 diabetes who attend public hospital clinics in sub-Saharan Africa, may look well, but they will need screening for CKD. The WHO document of Wilson and Jungner (53)support CKD screening amongst patients with type 2 diabetes because it is a public health problem, early disease is recognizable, screening tests are acceptable to populations, amongst its ten items. Indeed screening for chronic kidney disease in diabetes has been recommended but in the developed world (54, 55, 56). A review from experts to justify the same for overall CKD screen in sub-Saharan Africa was recently published. (57) Screening for a disease demands availability of (or access to) treatment and that is our major undoing in sub-Saharan Africa. Improved public health systems by governments, however should equalize opportunities for access to quality care, in this context, of high-risk diabetic patients like these in our study. The audit part of this study has been published (58). However, that spot urine test for albuminuria and occasional kidney function test for eGFR are not often done on these clinic attending patients, as standard of care, this paper was done to unmask the clinical information missed out on them.
Governments must therefore endeavor to enable public health systems or hospitals to improve the quality of diabetes care they offer. This includes enhancing the level of clinical care, deliberately screening for and case-finding of chronic kidney disease and then link, provide and retain them in appropriate care that should consequently forestall the more costly ESRD or cardiovascular events and/or mortality. Screening for CKD and case-finding without linkage to clinical care for control of risk factors and its management is an exercise in futility.
{kind=link}
{kind=link}
{kind=link}
{kind=link}