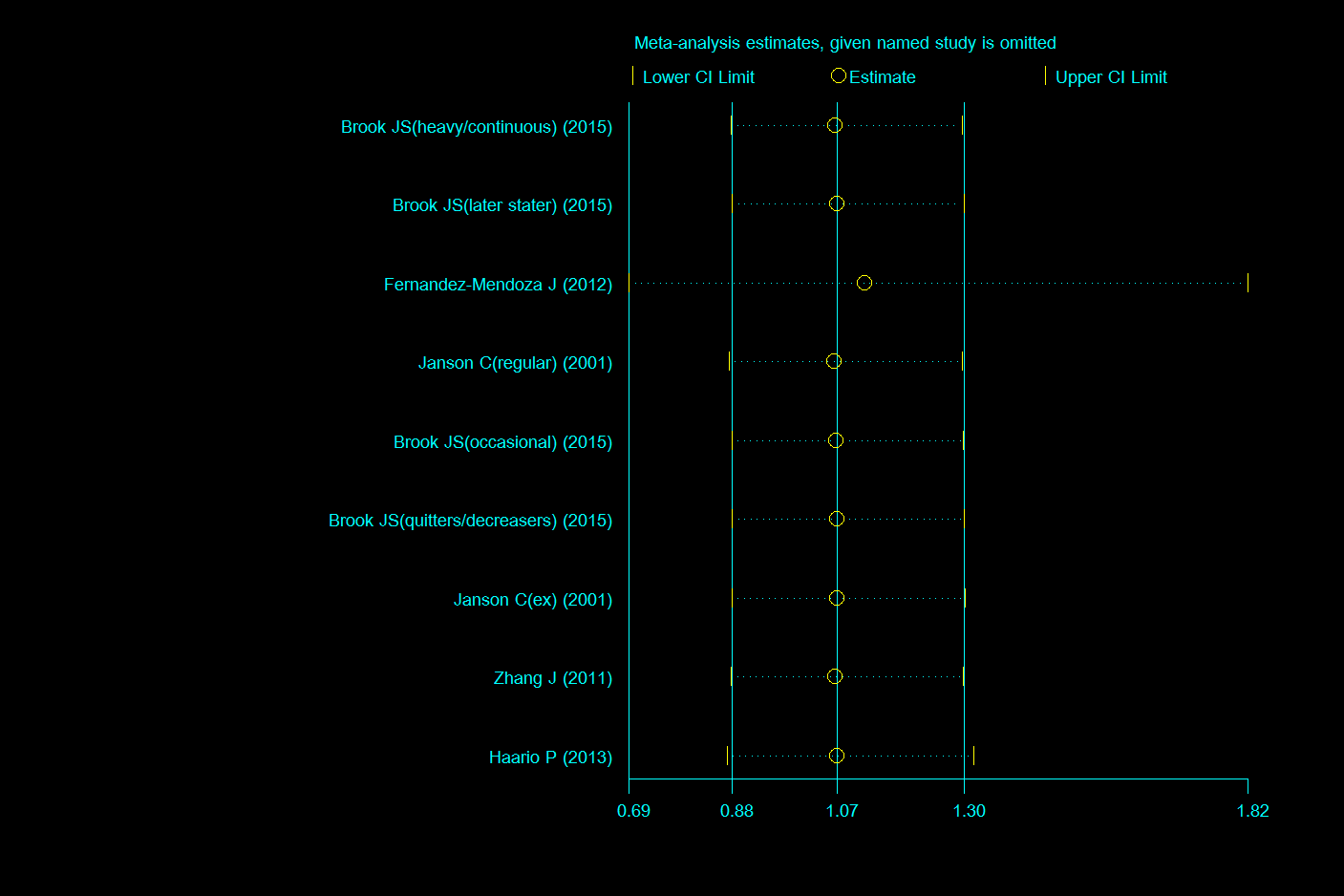
In this systematic review and meta-analysis, we quantitatively summarized available results from five cohort studies including about 12.5 thousand people to reveal the substantial association between smoking and incidence of insomnia. The results showed that smoking was significantly associated with incidence of insomnia. The heterogeneity was not considerate and was mainly from one study [31].
4.1 Association between smoking and incidence of insomnia
Consistent with our result, several cross-sectional studies and epidemiological investigations suggested that smoking might be an independent risk factor for insomnia [19, 20, 35]. However, the difference in incidence of insomnia between smokers and non-smokers was very small (OR=1.07) which might limit the public health implications of the result. Firstly, since about 30% people might suffer from insomnia [1] and billions of dollars were spent on it [2-4], a small improvement of sleep health though anti-smoking could also create considerate public health benefits. Secondly, it was reported that insomnia was a risk factor of smoking among students [36] and there might be a vicious circle between smoking and insomnia [37], which further improved the meaning of understanding the relationship between smoking and incidence of insomnia.
For more specific and quantized results, we further conducted the stratified analysis by smoking status. The results showed significant association between regular smokers and incidence of insomnia. Several previous studies reported similar association[23, 35]. The association between occasional smokers and incidence of insomnia was not significant. The main cause of smoking’s negative effect on sleep is associated with chemicals in it, so after quitting or decreasing, the impact might reduce. However, one study demonstrated that sleep architecture disturbances among current smokers were not influenced by the amount of smoking quantified by pack-years [38], which indicated there might be other mechanisms of smoking’ impact on sleep. Besides, it was reported that occasional smoking was significantly associated with excessive daytime sleepiness while regular smoking was not [39]. Firstly, there were only three cohorts in the regular-smoking subgroup and the heterogeneity was minimal. Therefore, we confirmed the result was credible. There was only one included study in the occasional subgroup which might cause the bias. Secondly, since the effects of smoking were associated with nicotine-acetylcholine receptors in our brain [38], as the daily amount of smoking increased, this kind of receptors might be saturated at some point and the effects of smoking might reach the maximum. The effects of nicotine on our brain were nonspecific, so while its concentration in the blood reached a certain value, other effects might gradually emerge which could alleviate the effects of nicotine on sleep health. There is still no satisfied explanation based on existing studies. More work on the association between the amount of smoking quantified by pack-years and insomnia were needed to be done. To better understand the etiology, concentration of nicotine and other chemicals in cigarette needed to be tested among insomnia population so their effects on sleep could be analyzed.
The pooled analysis didn’t indicate a significant association in ex-smokers. It was also reported that there were not significant differences between former smokers and never smokers for the prevalence of trouble sleeping[40]. Another study showed that longer sleep duration was associated with successful smoking cessation[41]. All these suggested that quitting smoking might be beneficial to sleep health and current smokers might improve sleep quality by quitting smoking.
4.2 Subgroup analysis
The region-specific analysis found significant association between smoking and incidence of insomnia in North America and Asia. Epidemiological investigations and cross-sectional studies in these places reported similar conclusion[6, 18]. However, the Asian subgroup included only one study and focused on insomnia in adolescents around 13 years old. We needed to be cautious about the result as the age difference of the participants might result in the inhomogeneity. The association was not significant in Europe. Consistent with our result, several prior studies[25, 42] showed that there was no significant association between smoking and insomnia in Europe. Differences in living habits, social atmosphere and gene might contribute to the different results between areas. We noticed that Mediterranean diet, which was popular in Europe, was possibly beneficial factor for sleep health[43]. The pace of life in Europe was much slower than in other areas and lifestyle has been reported to related to insomnia[5]. Besides, genetic diversity might also have an influence on how human organism reacted to chemicals in cigar[44]. Therefore, it is possible for people to avoid insomnia by changing living habits including diet or slowing down the pace of live.
Subgroup analysis based on age suggested significant association both in adults (>18) and juveniles (≤18). Similar results were reported by other studies[7, 45, 46]. Considering only one included study focused on juveniles, the result might be influenced by region and smoking status which was associated with the effect of smoking on insomnia as discussed above. More work remained to be done to reveal the association between smoking and insomnia in juveniles. A cohort study of the unborn reported the adverse influence of in utero exposure to smoking on sleep patterns in preterm neonates[47], which suggested that smoking might influence sleep health at a very early age. Therefore, people of all ages should try to avoid smoking for improving the sleep health.
Because included studies didn’t divide participants into males and females, we couldn’t conduct a subgroup analysis based on gender. To explore whether gender was associated with insomnia in smokers, we divided included studies into subgroups by gender ratio (women/men). The result suggested significant association in population with gender ratio (women/men) <1, but not in population with gender ratio(women/men) ≥1, that is, smoking has a negative influence on sleep in population which males are more than females. The point was reported for the first time. Prior study suggested that females were more likely to suffer from insomnia[24]. After discussion, we concluded that as male smokers were more than female smokers, the sample size of female smokers was not enough in included studies, which might contribute to bias. Wetler et al (1994)[48] suggested that both for males and females, current smoking was associated with several kinds of insomnia symptoms. The association was not significant when we changed the endpoints to other insomnia symptoms. Besides, the frequency of insomnia symptoms had an influence on the association. The pooled result in population with gender ratio (woman/man) ≥1 showed a high heterogeneity and one reported significant association between smoking and incident insomnia, the other didn’t. As there were only two studies in the subgroup, different region, mental disorder and social status might all contribute to the high heterogeneity, which reduced the credibility of the result. Passive smoking has also been found to associate with sleep disturbance among pregnant women[49]. To better understand the interaction between gender, smoking and insomnia, more work with female smokers and comprehensive analysis of all-cause insomnia incidence remained to be done.
- Biological mechanisms
Our study identified smoking, especially regular smoking as a risk factor for insomnia. The specific biological mechanism of smoking to particulate matters is still evolving. So far, nicotine, the primary addictive component of cigarettes or tobacco, was the most concerned. Nicotine has a known potential for enhancing attention and maintaining a certain level of arousal [50]. These effects are obtained by the central release of dopamine, norepinephrine, serotonin, acetylcholine, all of which have been implicated in the regulation of wakefulness, and by the stimulant effect that nicotine has on cholinergic neurotransmission in the basal forebrain responsible for cortical arousal[50]. In relation to insomnia, nicotine can regulate and change the normal neurotransmitter and disturb sleep architecture both in the early[38] and later stages of the sleep[48]. The changes have been detected by sleep parameters analysis (polysomnography, PSG). Furthermore, nicotine could generate a dose-dependent reduction in sleep efficiency, slow-wave-sleep, REM (rapid eyes movement) sleep and total sleep time[51, 52].
Besides, several psychosocial and physiological factors may account for the association between smoking and incident insomnia. Depression and obesity might be underlying factors in the biopsychosocial domain [5]. Cigarette use has been linked to adverse life events and work stress, which are also associated with insomnia symptoms[5]. Future studies are needed to investigate these multiple associations and reveal the biochemical relationship between smoking and insomnia.
- Strengths and limitations
There are several strengths in our study. Firstly, the five studies we included for meta-analysis and one for systematic review were all cohort studies. We did not include cross-sectional studies, because they couldn’t reveal the sequence of smoking and insomnia. Though there were several reviews of this topic, none of them included meta-analysis. So this article was the first systematic review and meta-analysis in the recent 20 years. Secondly, the quality of included studies were high or moderate, which might contribute to the reliability. Besides, we systematically analyzed the association between smoking status and insomnia, which provided extra basis for the public policy of promoting anti-smoking.
We admitted limitations in the following aspects. Firstly, the number of included studies is not enough, especially for subgroup-analysis. Secondly, the pooled result of smoking and incident insomnia in population with gender ratio (woman/man) ≥1 showed a high heterogeneity. There were two studies in this subgroup and one suggested significant association and the other didn’t. Excluding any one of them showed different consequences. Thirdly, insomnia includes different kinds of symptoms. We didn’t find enough studies on specific insomnia symptoms to conduct subgroup analysis while studies focused on different insomnia symptoms might have different results. Besides, insomnia might be a predictive factor for smoking behaviors and we didn’t conduct a further discussion due to the limited number of relevant studies. Lastly, alcohol, tea, social status, depression and other factors might also have an interaction with smoking and insomnia, which were not discussed in the study.
- Recommendations for future studies
7.1 Study design
We suggest high-quality longitudinal studies and cohort studies with detailed baseline information and regular health examination as ideal study method. Population with different features, such as a specific job or different age groups and gender composition, should be recorded and synthesized by stratified analysis. Mental health, geographical region and other potential factors should be taken into account to improve the representativeness of the study.
7.2 Smoking status
Future studies should record daily cigarettes that participants smoke and divide them into different groups. The association between smoking and insomnia need more quantification.
7.3 Adjustment by covariates
During the review of eligible studies, we found various covariates which may exert unstable impact on the summary. We recommend standardized covariates included at least age, sex, BMI, smoking status, alcohol consumption, chronic respiratory diseases, mental disorder, socioeconomic status at an individual level. Further adjustment can be performed by personal habits (such as physical activities, diet) and health status (such as diabetes, family history of disorder). This work requires detailed and elaborate baseline information.
7.4 Definition of endpoints
Though all studies provided definition and diagnostic criteria, some studies lacked preciseness when describing insomnia. We recommend future studies definite insomnia according to DSM. And more studies are needed to discuss the relationship between smoking and specific insomnia symptoms.
{kind=link}
{kind=link}