Between 2012 and 2018, there were 33 193 TB cases reported to the Sabah State TB surveillance database (myTB). This equated to an overall notification rate of 128 cases (range: 120–133) per 100 000 population (Figure 1), and 19.7% (range: 18.9–20.1%) of the total reported TB burden nationally in Malaysia.
TB case numbers and notification rates varied substantially between the 25 districts of Sabah. Kota Kinabalu, the state capital and largest population centre of Sabah, had the highest annual number of TB cases in each study year (n = 904 in 2018), accounting for 15–18% of reported cases. The highest case notification rates were seen in the Eastern coastal district of Semporna and northern coast district of Pitas, both with 228 cases per 100 000 population in 2018. The lowest reported rates in 2018 were in the central eastern district of Kinabatangan (56 cases per 100 000) and interior district of Tongod (53 cases per 100 000), both of which are characterised by large areas of jungle and remote rural communities (Figure 2).
Demographic characteristics
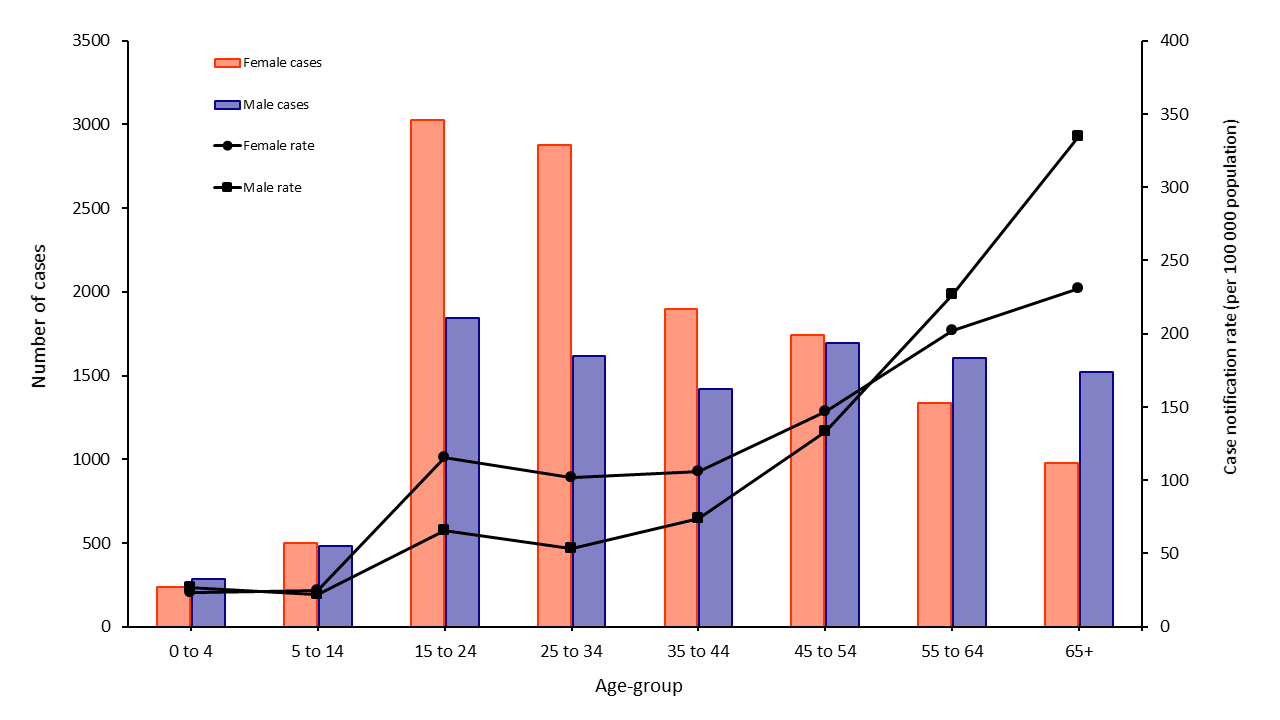
The median age of TB cases was 38 years. Case notification rates increased steadily with age from a low of 23 cases per 100 000 among children aged 5–14 years, to a high of 402 cases per 100 000 among adults aged 65 years and older. Only 1.6% of cases were among children aged less than five years, and 4.6% of cases were children less than 15 years. Further, the proportion of total cases that were children decreased from 2012 to 2018: by 2018, only 1.2% of cases were < 5 years and 3.6% were < 15 years.
There was substantial gender disparity among reported TB cases; 60% of cases were male. This was most notable in older age groups – in particular, those aged ≥ 55 years had a male to female notification ratio of 2.1꞉1. In both males and females, notification rates increased with age, but from adults aged 25 years and older, there was increasing disparity between sexes. The highest notification rates were seen in males aged 65 years and older at 540 cases per 100 000 population (compared to 254 cases per 100 000 in females in the same age group). There was little difference in the number of notifications between males and females among children less than 15 years (Figure 3).
Over the course of the study period, 50% of cases were born in Malaysia. Of cases born outside Malaysia, the majority were born in the Philippines (17%) and Indonesia (7%). The remaining 26% represented a range of other nationalities. There was some variation in the distribution year to year, though no obvious trend (Figure 4). Most cases (71%) were Malaysian citizens, and no trend in the proportion of cases with or without Malaysian citizenship was observed over the study period. However, there was a substantial difference by district of residence in the proportion of cases who were non-citizens – ranging from < 5% of cases in Nabawan, Kota Belud and Pitas, to > 50% of cases in the eastern districts of Lahad Datu and Kunak and 62% of cases in Kinabatangan (Figure 5). Among overseas-born cases, only 14% had been in Malaysia < 5 years at their time of diagnosis; 52% of overseas-born cases had a length of stay in Malaysia of 10–29 years at their time of diagnosis.
Over the study period, monthly median household income of TB cases was 1000 Malaysian Ringgit (MYR) (equivalent to ~USD 250).
Case detection and diagnosis
Overall, 57% of TB cases were diagnosed in Government hospitals, with 42% diagnosed in public primary health or village clinics and 2% diagnosed in private facilities. Over time, there was a decrease in the proportion of cases diagnosed in government hospitals, from 61% of cases in 2012, down to 52% in 2018. A corresponding increase in diagnoses occurred in primary care (primary health and village clinics) and a small increase at private facilities (clinics and hospitals). (Figure 6).
Between 2012 and 2018, most cases (89%) were detected passively. Of those that were diagnosed through active case finding, 74% (n = 2244 cases) were detected during contact investigation – equivalent to 6.8% of all TB cases during this period. The remaining 26% of cases were detected through various screening mechanisms, such as community or occupational screening – equivalent to 4.2% of all TB cases during this period. The overall proportion of TB cases detected through community screening did increase from 2014 onwards, though accounted for only a very small proportion of overall case detection (reaching just 1.7% in 2018).
Seventy-three percent of TB cases between 2012 and 2018 were bacteriologically confirmed (range 70–74%). However, among children less than five years, only 19% were bacteriologically confirmed. Among all cases during this period, only 74% were tested by culture, varying year to year from 51% to 87%. Culture positivity was low at 24% overall, ranging from 11% to 29% between years. Culture positivity among pulmonary cases only was 26%. A total of 403 cases were tested by GeneXpert® during the study period, equating to test coverage of only 1.2% (range: 0.3–3.0%). GeneXpert® positivity was higher than culture at 66% overall, but also varied substantially from 0% (of 12 samples tested) in 2012 to 89% (of 149 samples tested) in 2016. Most cases (97%) had smear microscopy results available, and this was consistent across the period. (Table 1).
Table 1: Diagnostic results of notified TB cases by year, Sabah, 2012–2018
|
Year
|
Bacteriologically confirmed
|
GeneXpert®
|
Culture
|
Smear microscopy
|
|
Number of cases tested
|
Proportion of cases tested
|
Proportion of tests positive
|
Number of cases tested
|
Proportion of cases tested
|
Proportion of tests positive
|
Number of cases tested
|
Proportion of cases tested
|
Proportion of tests positive
|
|
2012
|
74.3%
|
12
|
0.3%
|
0.0%
|
2232
|
50.8%
|
11.3%
|
4227
|
96.3%
|
76.6%
|
|
2013
|
73.1%
|
15
|
0.3%
|
6.7%
|
3223
|
71.2%
|
13.5%
|
4363
|
96.4%
|
75.1%
|
|
2014
|
72.8%
|
27
|
0.6%
|
29.6%
|
4108
|
86.5%
|
22.4%
|
4598
|
96.9%
|
74.5%
|
|
2015
|
74.0%
|
80
|
1.8%
|
41.3%
|
3620
|
81.1%
|
28.4%
|
4328
|
97.0%
|
75.3%
|
|
2016
|
74.1%
|
149
|
3.0%
|
88.6%
|
3971
|
80.2%
|
29.2%
|
4827
|
97.5%
|
74.0%
|
|
2017
|
70.0%
|
74
|
1.4%
|
71.6%
|
3981
|
78.0%
|
28.6%
|
5016
|
98.3%
|
69.8%
|
|
2018
|
70.0%
|
46
|
0.9%
|
82.6%
|
3375
|
67.4%
|
26.1%
|
4904
|
97.9%
|
70.5%
|
|
Total
|
72.6%
|
403
|
1.2%
|
65.8%
|
24 510
|
73.8%
|
23.7%
|
32 263
|
97.2%
|
73.5%
|
Among pulmonary cases, sputum smear positivity at diagnosis was high at 81% between 2012 and 2018, however there was a decreasing trend in sputum smear positivity from 84% in 2012 to 79% in 2018. When broken down by citizenship status, 85% of non-citizens with pulmonary TB were sputum smear positive at diagnosis, significantly higher than the proportion of Malaysian citizens (79%) who were smear positive at diagnosis (χ2 = 145.9, P < 0.0001).
Chest X-ray coverage of pulmonary cases was high across the study period, with 97% of cases having a chest X-ray finding at diagnosis recorded. Fifty-one percent of pulmonary cases had moderately advanced (44%) or far advanced (6%) disease at diagnosis, with the remaining 49% having minimal lesions or no lesion present on chest X-ray. Malaysian citizens were significantly less likely to have moderate or advanced disease (46%) on chest X-ray at diagnosis compared with non-citizens (57%) (χ2 = 362.7, P < 0.0001).
Case classification
Of the 33 193 cases notified between 2012 and 2018, 94% were new TB cases and 6% were reported as previously treated (range: 5.4–7.2%). Eighty-nine percent of cases had pulmonary disease, with the remaining 11% having extrapulmonary disease only. There was no change over time in the proportion of extrapulmonary TB. Among 4166 cases of TB with extrapulmonary involvement reported between 2012 and 2017, the most common sites of infection were the lymphatic system (33%), pleura (17%), bone, joints and soft tissue (15%), and gastrointestinal system (13%). Ten percent of cases had central nervous system disease, including TB meningitis, and 7% with extrapulmonary involvement had disseminated disease. The genitourinary system, pericardium and eyes accounted for very small numbers (< 2%).
Risk factors
Overall, 7% of TB cases were recorded as having diabetes, increasing from 5% of cases in 2012 to 8% in 2016–2018. There was no difference in diabetes prevalence by gender. Just under one-third of TB cases (31%) were recorded as smokers, the prevalence of which remained unchanged. The proportion of cases who smoked varied greatly by gender, with 48% of male TB cases recorded as smokers, versus just 4% of female cases recorded as smokers. Among those aged 35 years and older, the male to female ratio decreased from 2.0 to 1.1 when smokers were excluded. (Supplementary figure 1) An average of 48 cases of TB per year (approximately 1% of cases) occurred in healthcare workers. HIV testing among TB cases was high, with results of HIV testing recorded for more than 99% of TB cases. HIV prevalence among TB cases was low, with just 1.8% of cases between 2012 and 2018 recorded as having HIV co-infection (range: 1.6–2.0%). Among TB cases with HIV co-infection, 43% received antiretroviral therapy (ART) (range: 29–63%).
Drug resistance
A total of 87 cases of MDR-TB were reported in Sabah between 2012 and 2018 (range: 9–16 cases per year), equivalent to 0.3% of all cases. MDR-TB prevalence was 0.1% (n = 42) among new cases and 2.2% (n = 45) among previously treated cases. One-third of MDR-TB cases occurred in just two districts, Kota Kinabalu (17%, n = 15) and Tawau (16%, n = 14).
Treatment outcomes
Treatment success among cases of drug-sensitive TB was 83% (range: 81–85%) for the period of 2012 to 2018. Less than 1% of cases failed treatment and 8% of cases died. Among the remainder, 2% of cases were recorded as lost to follow-up and 6% of cases were not evaluated. There was no substantial change in treatment outcome among drug-sensitive cases over the study period. Among cases of drug-sensitive TB, 84% of new cases successfully completed treatment, versus 77% of previously treated patients. Among cases of MDR-TB, treatment success was much lower, with only 36% (range: 25–45%) of cases reported between 2012 and 2016 cured or successfully completing treatment. Three percent of MDR-TB cases died, 31% failed treatment, and 7% were lost to follow-up. The remainder were not evaluated for treatment outcome. Given the small number of MDR-TB cases, it was not possible to determine any trend in treatment outcomes over time.
{kind=link}