Patients and treatment management
For testing the eDOTS system used in villages, we selected Yinjisha County of Kashgar Prefecture in southern XUAR. Two communities with 95% of villager being Chinese Uygur were selected for respectively using DOTS and eDOTS. Considering the cross impacting between villages with the two treatments, the distance of villages with different managements was at least 10 km apart from each other. One villager doctor looked after the whole PTB patients in a village with a total 13 villages involved. For testing the treatment management in township, we selected TB patients from residential communities in Urumqi city area,where one community doctor was in charge of a community.
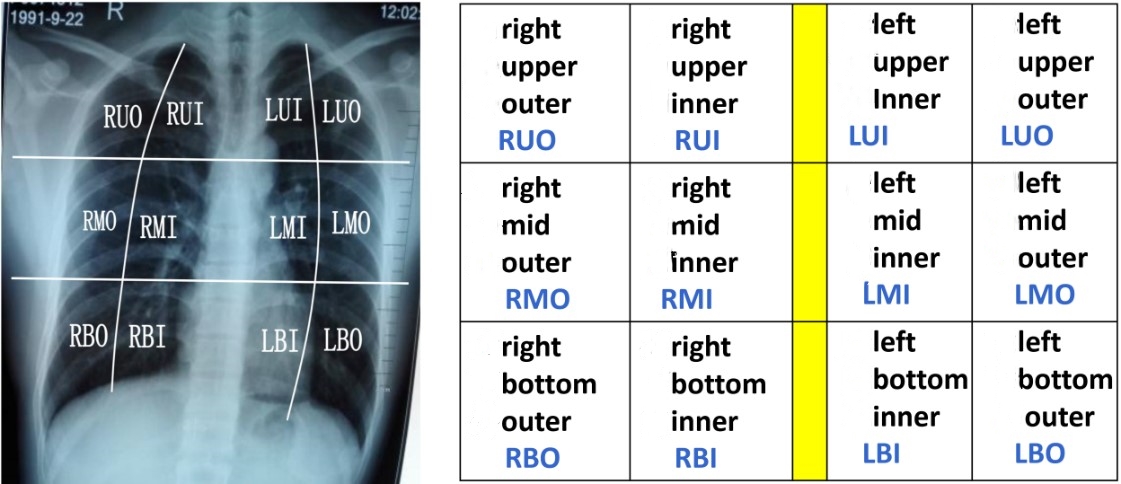
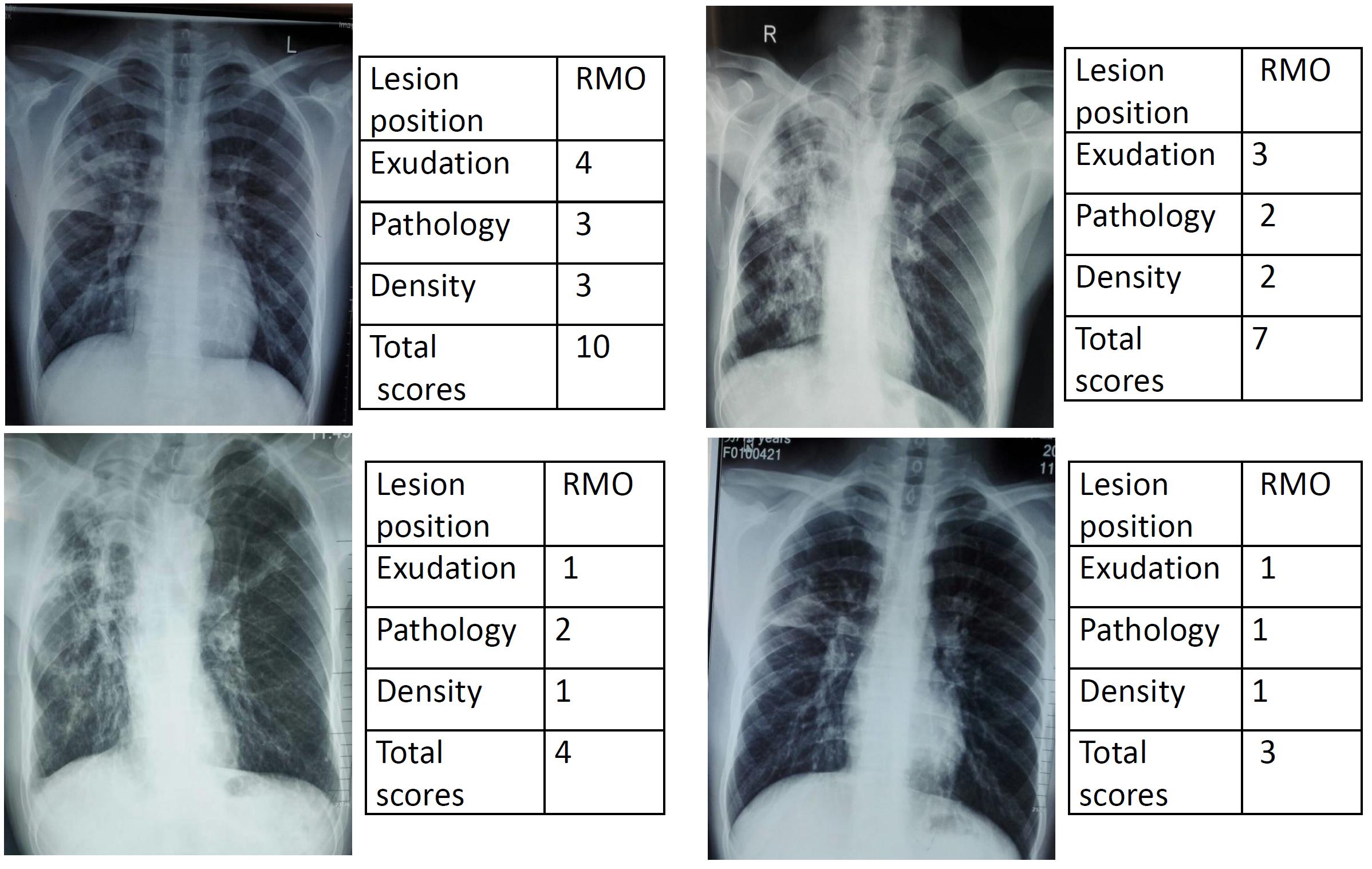
PTB patients aged between 15 and 75 were randomly selected by the timing of diagnosis. Pregnant women and patients with HIV infection or using hormone were excluded. Most of the PTB patients were diagnosed through annual health check program referring to the criteria [13] published by the Ministry of Health of China. All the patients showed DR (Digital Radiography) positive with clear and typical symptoms such as night sweats, chest pain, persistent cough and fever for two weeks with some coughing up blood sputum. In addition, we established a DR scoring system for evaluating the TB status mainly according to DR chest radiograph. TB lesion image features were classified into three levels based on lesion image features including exudation areas (3 scores), pathology including proliferation (4 scores) and infiltration and density of TB lesion (3 scores) (Supplementary data 1). Three X-ray experts were asked to score the TB lesion progress for each of the patients. Examples are shown in Fig. S1 and S2.
The study was reviewed and approved by the Ethic Committee of the First Affiliated Hospital of Xinjiang Medical University with approval No. ( 20150824-01). All the patients involved in the project had an informed consent signed.
Training plan
All doctors from villages and downtown communities and staff involved in the study had one-day training for introduction and use of the device and the system. Once a PTB patient was diagnosed and confirmed, he or she was registered as a TB patient in the study and recorded all possible information for DOTS treatment including name, ID, age, gender, family location, diagnosis information such as smear results, X-ray and treatment prescription etc. After registered, an eDOTS box and a week of anti-TB medicine were supplied. Doctors saw their patients once a week and added the drugs for the next week.
Drug treatment
Standard anti-TB drug combinations containing isoniazid (H), rifampicin (R), pyrazinamide (Z), ethambutol (E) were applied for those PTB patients according to WHO recommendation as the first line anti-TB drugs [14]. Two treatment courses for all the cases include a two-month intensive phase with a daily dose of fixed-dose combination tablets containing HRZE, followed by a four-month continuation phase of daily HR [15].
Data records
The eDOTS system recorded the patient’s medication activity and automatically transferred into the management system in CDC. If a patient did not take the medicine in time, the system automatically transferred a message to her/his doctor and relative asking them to remind the patient taking the medicine. If the patient was still not taking the medicine after 5 pm in the day, the system recorded as “non-taking medicine”. In DOTS group, doctors were normally ticking on the book for taking or not taking medicine. Results
Intervention treatment
A total of 167 active TB patients were registered from 14 villages from 2 communities in Yinjisha County of Kashgar and 2 districts in Urumqi city, XUAR. Ninety-three patients were treated with eDOTS and 74 with DOTS. In eDOTS group, only 3 patients fully and completely took the treatment during the treatment course, that was 8% of the total patients after 6 months of treatment course. The most patients did not fully take their medicine for some of reasons including neglect of medication, drug side effect, visiting friends. However, the doctors responsible for DOTS in both rural and downtown area all claimed that 100% of all 74 enrolled cases were on medication every day during the intervention.
Treatment in the villages
Eight-one patients (Uygur ethnic) from villages were enrolled in a time course of being diagnosed with 43 patients from 9 villages treated with eDOTS system and 38 patients from 5 villages using DOTS as control.
In the first 6 weeks of management in the eDOTS group, the average medication compliance rate was 48.8%, 95% CI (46.5%, 51.1%). At week 7, the network was accidently disconnected and DOTS had been supplied for those eDOTS patients for two weeks. However, when the system was reused, the compliance rate was dropped to 27.9%, 95% CI (22.8, 33.0%). We then asked the village doctors to closely contact with those patients and the rate for taking drugs was increased to 65.1%, 95%CI (59.7%, 70.5%) at week 20 subsequently. After we then asked a well trained doctor from a hospital to contact with those patients who did not take drugs, the average medication compliance rate was increased to 77.2%, 95% CI (75.1, 79.3%) (Fig. 2).
Treatment in the township
We used the eDOTS for 50 patients (Han ethnic 34, Hui ethnic 16) compared with 36 patients (Han ethnic 28, Hui ethnic 8) using DOTS in Urumqi city. Those 50 patients were monitored by one community doctor with his mobile phone or laptop through the system.
In the first 12 weeks of the intervention, the compliance rate of the patients with eDOTS was almost 100%. After 12 weeks, the rate was slightly dropped, but the overall compliance rate was kept in more than 80 percent (Fig. 3).
The first 6 weeks of treatment of patients with eDOTS showed that village patients had 45-55% of compliance taking anti-TB drugs, which was significantly lower than the compliance rate of patients in township (99-100%) (Χ2=193.445, P<0.01).
DR X-ray score analysis
There was no statistic difference on TB scores from patients between town and villages which were both 9.1± 1.3 points before treatment. Whether DOTS or eDOTS was used, TB scores can be significantly reduced in both downtown and rural area at the end of the intervention period (Fig. 4). We analyze the scores by using two-way ANOVA with Tukey's multiple comparisons test after 25-26 weeks of treatment. TB score (3.5±0.6 points) of patients from Urumqi with eDOTS was significantly lower than those (4.5±1.6) with DOTS by 1.1points [95% CI (0.2, 2.0), q=5.036, p=0.05<0.01]. In village, TB score (4.2±0.6 points) of patients with eDOTS was lower significantly than those (6.0±1.6) with DOTS by 1.8 points [95% CI (0.5, 3.1) , q=6.052, p<0.01]. Comparison after using eDOTS, there was no difference between the score (3.5±0.6 points) of TB patients in downtown and those (4.2±1.2 points) in rural areas (q=2.596, p>0.05). Comparison only after using DOTS, the TB score (4.5±1.6 points) of patients in downtown was lower significantly than those (6.00±1.5 points) in village by 1.5 points [95% CI (2.5, 0.5), q=6.339, p<0.01)].
{kind=link}
{kind=link}