Snoring, the manifestation of increased upper airway resistance, is commonly regarded as a reliable proxy marker of obstructive sleep apnea(OSA)[1, 2].Moreover, regular snoring has been suggested to be correlated with obesity[3], hypertension[4] and diabetes mellitus[5]. Since OSA is supposed to be more prevalent in men than women, the gap was narrowed when women approach menopause[6, 7]. In addition, previous studies have reported that menopause was an important risk factor for snoring[8, 9].
Menopause is well documented as an essential physiological stage of women's lives with vasomotor symptoms[10], sleep disorder[11] and etc. Meanwhile, menopause is a vital window for variations in the body composition and rising in the body weight caused by hormonal alterations[12]. However, body mass index, BMI, is not a valid measure of true obesity status in menopausal women[13].Changes in menopause-related body composition may be covered and underestimated by stable BMI since the counteractive effect of loss of lean mass and gain of fat mass when aging. Therefore, body composition by bioelectrical impedance analysis (BIA) may be a more representative and precise instrument rather than BMI among menopausal Chinese women[14].
So far, current studies on the association of snoring and obesity have focused primarily on men and children[3, 15],while underrepresented women. In addition, any association between snoring and body composition in menopausal women has received little attention. Since it's possible that glycolipid metabolism may confound the association, and whether snoring is associated with body composition in menopausal women independently of glycolipid metabolism confounders remains unknown. Given the evidence of the cross interplay among snoring, obesity and menopause, we aim to explore the association with snoring and body composition in menopausal women.
Subjects and methods
Study participants
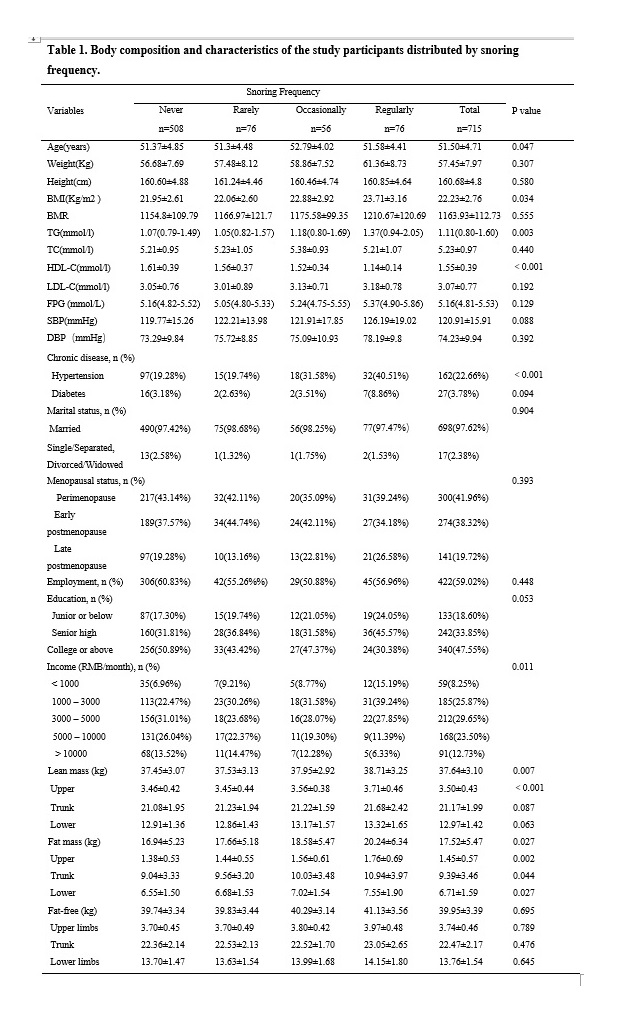
This cross-sectional study enrolled participants who visited the Menopause Clinic in the Shanghai Sixth People’s Hospital. Han-Chinese woman aged 40–67 years passing through the menopause were recruited. Exclusion criteria were (1) with rhinitis; (2) having severe internal illnesses and/or diseases such as myocardial infarction, stroke, and cancer; (3) current smoking (at least once per week for the previous 6 months); (4) excessive alcohol drinking (at least one pack per month for the previous 6 months); (5) suffering from thyroid disease; (6) having tubercle and cachexy; (7) missing data. Ultimately,715 participants were recruited in this study. All participants given the informed consent after full explanation, which was approved by the Institutional Review Board of Shanghai Sixth People’s Hospital"2016-R07".
General questionnaire
Baseline sociodemographic information was collected from a questionnaire through face-to-face interview, which has been previously employed[11]; Variables included age, marital status, employment status, education level, income per month, menopausal age, menopausal status, history of chronic disease (i.e., hypertension, diabetes mellitus, rhinitis, other diseases), besides, lifestyle (i.e., smoke, alcohol consumption) were recorded. Guiding by the Stages of Reproductive Aging Workshop (STRAW +10)[16] ,participants were divided into three different menopausal subgroups, namely menopausal transition group (consecutive irregularities for over 7 days of menstrual cycle), early postmenopausal group (absence of menstrual periods for 12months -5 years) and late postmenopausal group (absence of menstrual periods for ≥ 5 years).Hypertension was defined by any prior diagnosis from the questionnaire or by the criteria recommended by the seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7)[17]. While diabetes mellitus was identified by FPG ≥ 7 mmol/L or received any treatment for diabetes according to the WHO criteria[18].
Snoring frequency assessment
Participants were asked by the question to assess the sleep snoring frequency, which was applied previously[19, 20]. “Over the past 4 weeks, did you snore? And if did, how many times per week?” and the options for responses were “never”, “rarely”, “occasionally”, and “regularly”, corresponding to “never”, “<1 night per week”, “1–2 nights per week”, and “≥ 3 nights per week”, respectively.
Anthropometric and lab tests
We measured and recorded participants' weight, height. Body mass index (BMI) was computed by dividing weight in kilograms by the square of their height in meters. We took the blood pressure for all participants on the right arm three consecutive times after 5-minute sitting (systolic blood pressure(SBP), diastolic blood pressure(DBP)). Blood samples were collected for the detection of serum concentration of triglyceride(TG), cholesterol(TC), high-density lipoprotein (HDL), low-density lipoprotein(LDL), and fasting blood glucose(FBG) after an overnight fast.
Body composition
We measured the body composition by BIA (TBF-418B analyzer; TANITA) of lean mass (LM), fat mass (FM), and fat-free mass (FFM), and each segment included upper /lower limbs, and trunk. We also recorded basal metabolic rate (BMR)concurrently[21]. The well-trained staff guided the participants to take off heavy clothes, socks and shoes, and hold the hand electrodes, standing barefoot in contact with footpad electrodes[22].
Statistical analyses
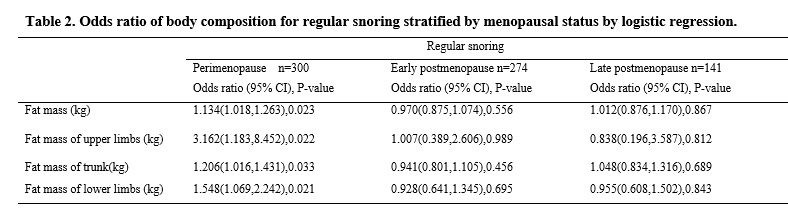
All statistical analyses were taken by SPSS 22.0 (IBM Corporation, Armonk, NY, USA). Data were tested for normal distribution by the Kruskal WallisH-test. Levene's test of homogeneity of variance was also performed. Variables were presented as mean ± standard deviation(SD)when they showed normal distributions, whereas medians (inter quartile range) or values (%). One-way ANOVA (normal distributions), the Kruskal Wallis H-test (skewed continuous variables) and χ2 test (categorical variables) were carried out to compare the differences among the four groups. Snoring was analyzed as a categorical variable with never as the reference group. Fat mass (total and each segment) and lean mass (total and each segment) were stated in the dichotomized form, with a cutoff of the highest quartile as the higher one (comparing the highest to the lower two tertiles). Relationship between body composition and snoring frequency was computed by multiple logistic regression analysis. Covariates included TG, TC, HDL, LDL, FBG, SBP, DBP, age, marital status, employment status, education level, income per month, menopausal age, menopausal status, hypertension, diabetes mellitus. Two-sided p<0.05 was considered significant.
{kind=link}
{kind=link}