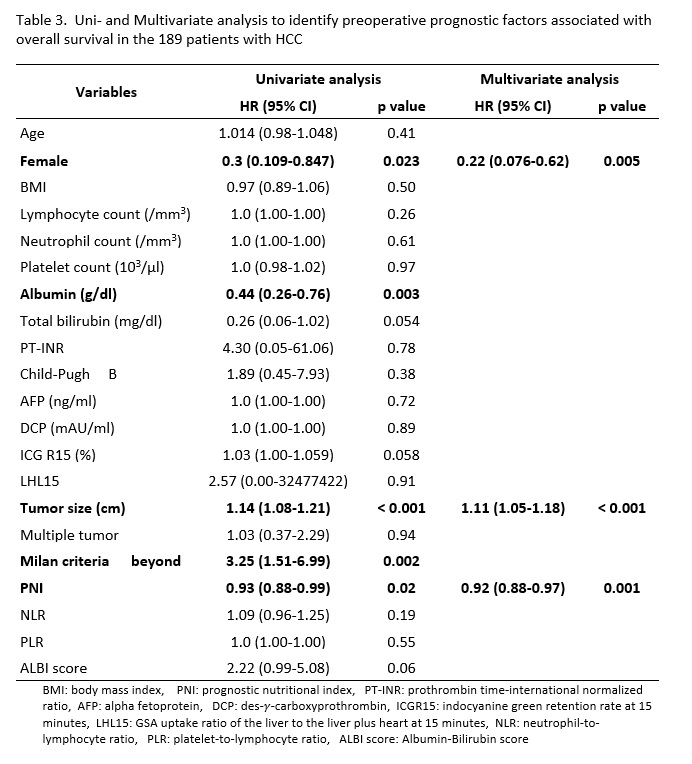
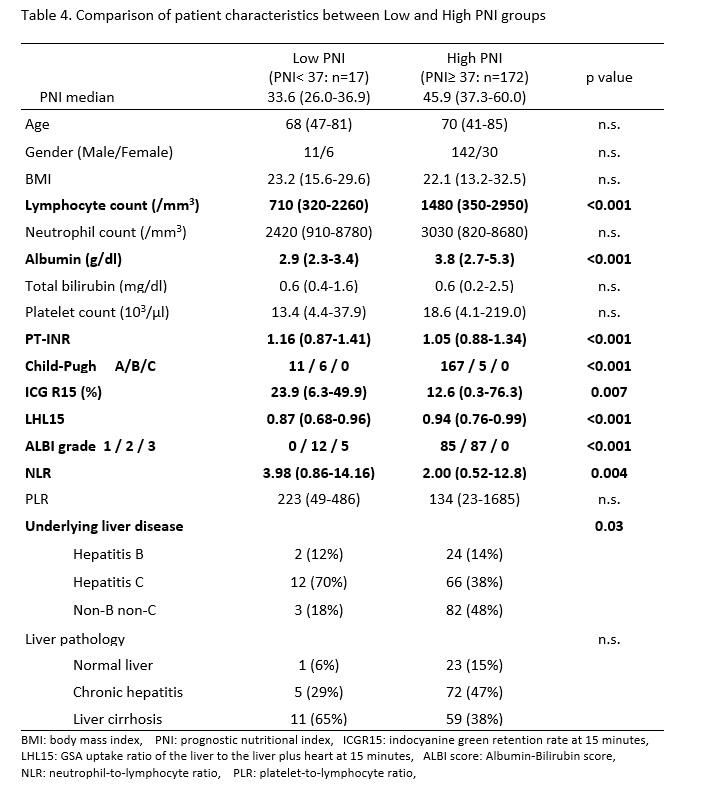
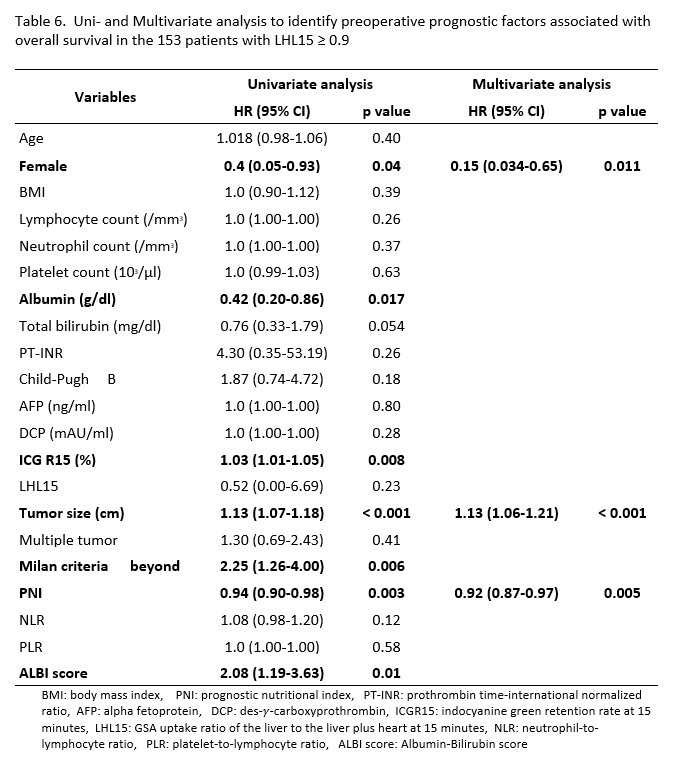
The present study determined that female gender, tumor size and PNI were independent prognostic factors for patients with hepatectomy for HCC without previous treatment. Other inflammation-based scores, such as NLR and PLR, were not independent prognostic factors. The optimum PNI cut-off value for OS was 37. Patients with a low PNI less than 37 had significantly impaired liver function, significantly poor prognosis and were immunocompromised. Even in patients who had preserved liver function with LHL ≥0.9, PNI remained an independent prognostic factor and showed significantly lower OS and PFS, which were not observed in patients with impaired liver function with LHL15 <0.9.
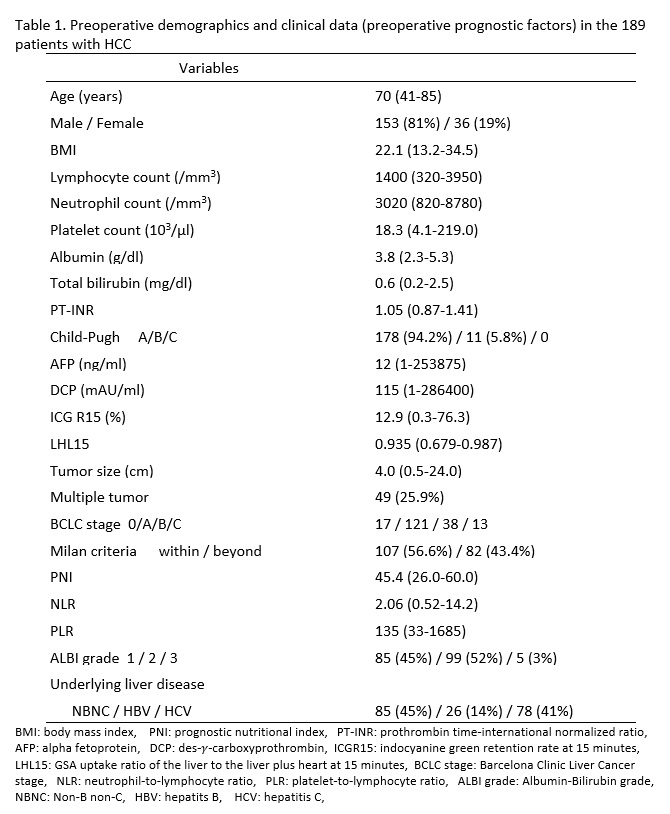
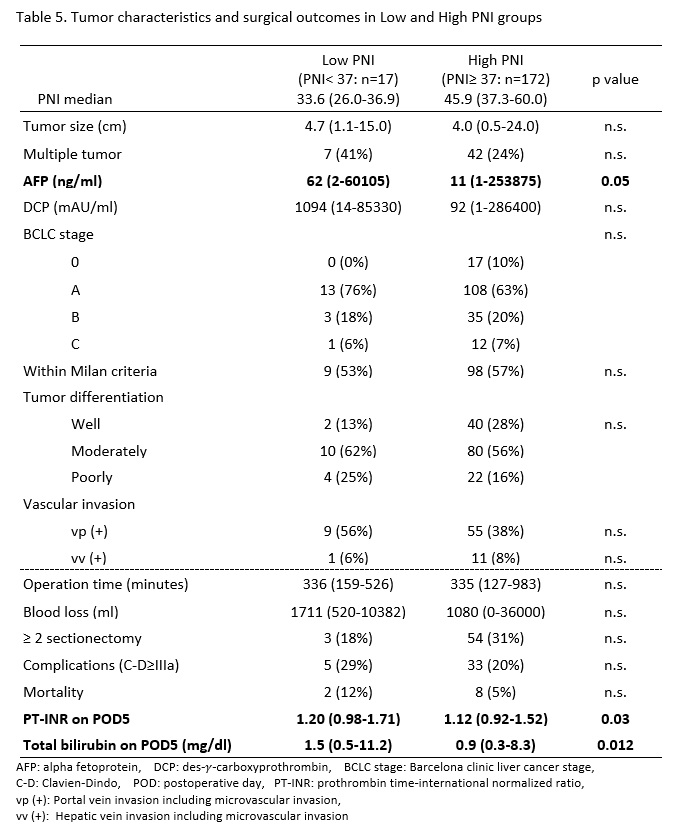
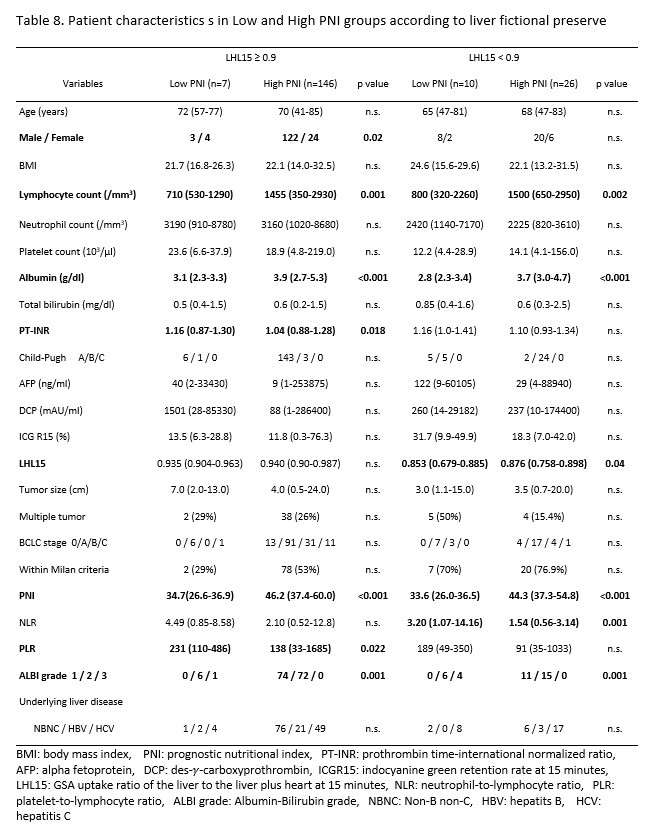
Although several previous studies indicated that PNI was a significant prognostic factor in HCC patients (13-21), these reports did not examine why low PNI correlated to the prognosis. Because PNI consists of albumin and lymphocyte levels, low PNI means hypoalbuminemia and lymphocytopenia, which may contribute to tumor development and progression. Lower albumin levels in patients with lower PNI reflects malnutrition and impaired protein synthesis ability in livers with chronic inflammation and fibrosis due to the underlying liver disease. Serum albumin level was integrated into several HCC staging systems, and a new albumin-derived score, ALBI score (24), predicted the prognosis of HCC patients. In the present study, the Low PNI group had lower survival and poorer liver functions and showed significantly higher PT-INR, ICGR15, a higher rate of Child-Pugh B and ALBI grade ≥2 and significantly lower LHL15. Chan AW et al. (14) revealed that a lower PNI (<45) group was associated with higher model for end-stage liver disease (MELD) score and a higher rate of Child-Pugh class B patients in early stage HCC patients. However, no previous studies examined the relationship between PNI and liver functional reserve tests, such as ICGR15 and LHL15. The ICG test and 99mTc-GSA liver scintigraphy are more beneficial to assess liver function in hepatectomy rather than the MELD score or Child-Pugh classification because these tests provide detailed liver functional data (23, 27). Lower PNI was significantly associated with a detailed liver function in our study and showed significantly higher ICGR15 and lower LHL15.
Lymphocytes are another component and immune factor of PNI, and these cells play an important role in HCC recurrence and progression. We found a relationship between PNI and AFP, but not the other tumor biological statuses as assessed using tumor stage or histological findings. In a meta-analysis to systematically review the association between PNI and HCC prognosis (21), PNI was significantly associated with AFP level, tumor size and TNM stages. The loss of CD4 (+) T lymphocytes strongly contributed to HCC development in a mouse model (28). A clinical study on resected specimens of HCC patients demonstrated that high densities of CD3 (+) and CD8 (+) T cells in the interior and margins of the tumor were significantly associated with a low rate of recurrence and a prolonged RFS (29). These findings indicate that host immune status with lymphocyte infiltration of the tumor is important to prevent tumor progression. The present study also examined lymphocyte-related markers, such as NLR and PLR, but these markers were not selected as an independent prognostic factors in multivariate analysis. PNI predicted the prognosis of HCC patient more precisely than NLR and PLR because the PNI contains albumin and lymphocyte levels as nutritional and immune factors.
Our study stratified the patient survival more clearly according to PNI compared to previous studies with the use of 37 as the cut off value. We determined 37 as the PNI cut-off value by comparing the survival curves stratified by various cut-off values from 35 to 50, and other studies of hepatectomized HCC used cut-off values that ranged from 45 to 53 (13-21). One previous report defined the low-PNI group as PNI<45, which had a significant adverse 5-year OS of 57% (n=84) vs. 82% (n=240), p=0.001 (14). Another study defined the low-PNI group as PNI<48.5, which had a significant adverse 5-year OS of 46.5% (n=122) vs. 76.5% (n=134), p=0.001 (15). In contrast, our study newly defined the Low PNI group as PNI< 37, which had a more significant adverse 5-year OS of only 13% (n=17) vs. 67% (n=172), p=0.001. When we compared PFS between the two groups, median PFS time in the Low PNI group was significantly shorter (8 months) than the High PNI group (25 months) (p=0.002). Therefore, we determined that a PNI of 37 was the most practical cut-off value in clinical settings. When encountering HCC patients with PNI <37, we should strictly consider their operative indication because they have a high risk of early recurrence after hepatectomy and poor prognosis. Preoperative immuno-nutritional management should be required to increase PNI when surgical resection is the sole curative treatment option.
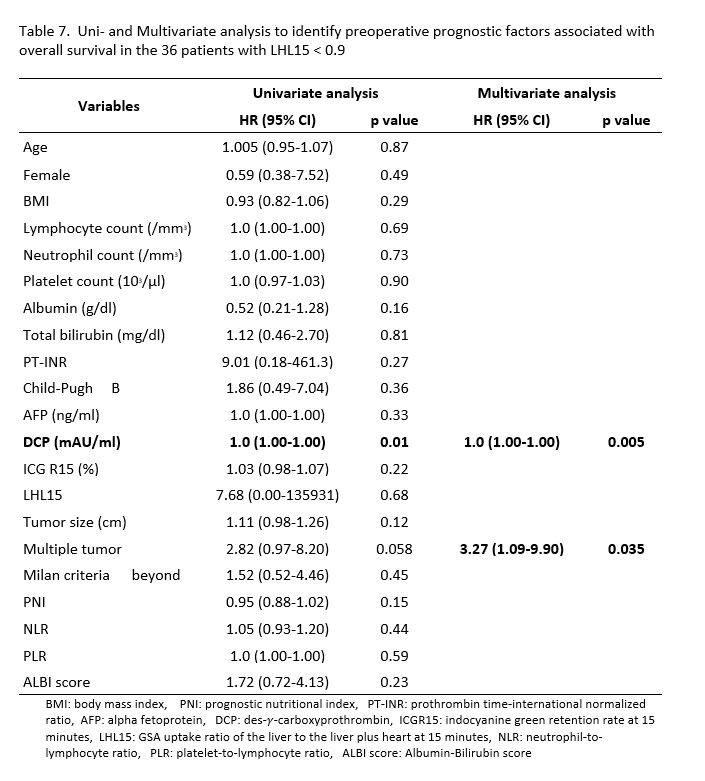
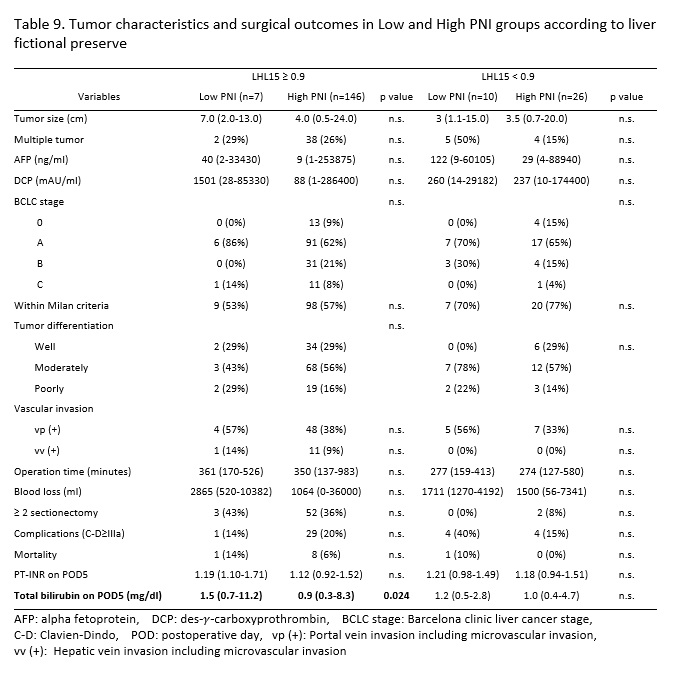
It is apparent that PNI is influenced by the liver functional reserve because a serum level of albumin is one component of PNI, and albumin is synthesized in the liver. Thus, we considered that in the subgroup of patients with preserved liver function, which means that the ability of synthesis of albumin is relatively preserved, PNI would more accurately reflect pro-tumor inflammatory and nutritional status than in those with impaired liver function. Therefore, we performed a subgroup analysis that adjusted for liver functional reserve. The patients were divided into subgroups according to liver functional reserve using LHL15. Multivariate analysis revealed that PNI still remained an independent prognostic factor in the subgroup with LHL15 ≥0.9 but not in the subgroup with LHL15 <0.9. In the preserved liver functional groups of LHL15 ≥0.9, the Low PNI group showed significantly lower OS and PFS than the High PNI group, but PNI showed no survival difference in the poor liver functional group of LHL <0.9. These findings demonstrated that PNI was a useful practical tool, especially in patients with preserved liver functional reserve, but not in the patients with poor liver function. PNI was proven to be a strong prognostic factor especially in the patients who had liver function preserved well, because it worked well even in the patient subgroup with preserved liver function of LHL15 ≥0.9. In the patients with poor liver functional reserve with LHL <0.9, tumor malignancy, such as high DCP level, and multiple tumors significantly affected patient survival more than PNI based on the multivariate analysis.
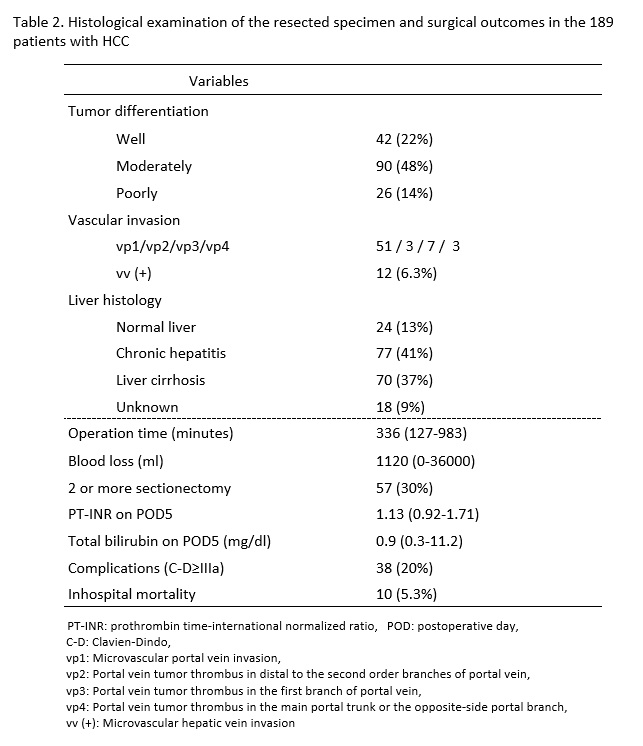
The results of our study showed that PNI may be used as a predictor of patient prognosis and an indicator for preoperative nutritional management. Preoperative nutritional treatment may be important for patients with PNI lower than 37 to increase albumin level and lymphocyte count because prognosis was extremely poor in patients with preserved liver functional reserve. Sarcopenia was recently correlated with postoperative complications and survival in HCC patients (30-32). To improve nutritional state and sarcopenia, preoperative nutritional intervention may be important. Nutritional intervention with branched-chain amino acid (BCAA)-enriched nutrient increased albumin levels and BCAA-to-tyrosine ratios before TACE for HCC patients (33). For the surgical treatment for HCC, perioperative enteral nutrition improved the recovery of gastrointestinal function, reduced morbidity and shortened the length of postoperative hospital stay (34, 35). In our study, postoperative complication rate was similar between the Low- and High PNI groups. However, the rate of major hepatectomy was higher in High PNI group than in Low PNI group. If surgical procedure is same in the two groups, poor nutritional status in Low PNI group may give the negative impact on postoperative course. The outcomes of preoperative management to improve PNI should be evaluated prospectively, including how preoperative nutritional support may improve PNI and surgical outcomes, including patient prognosis.