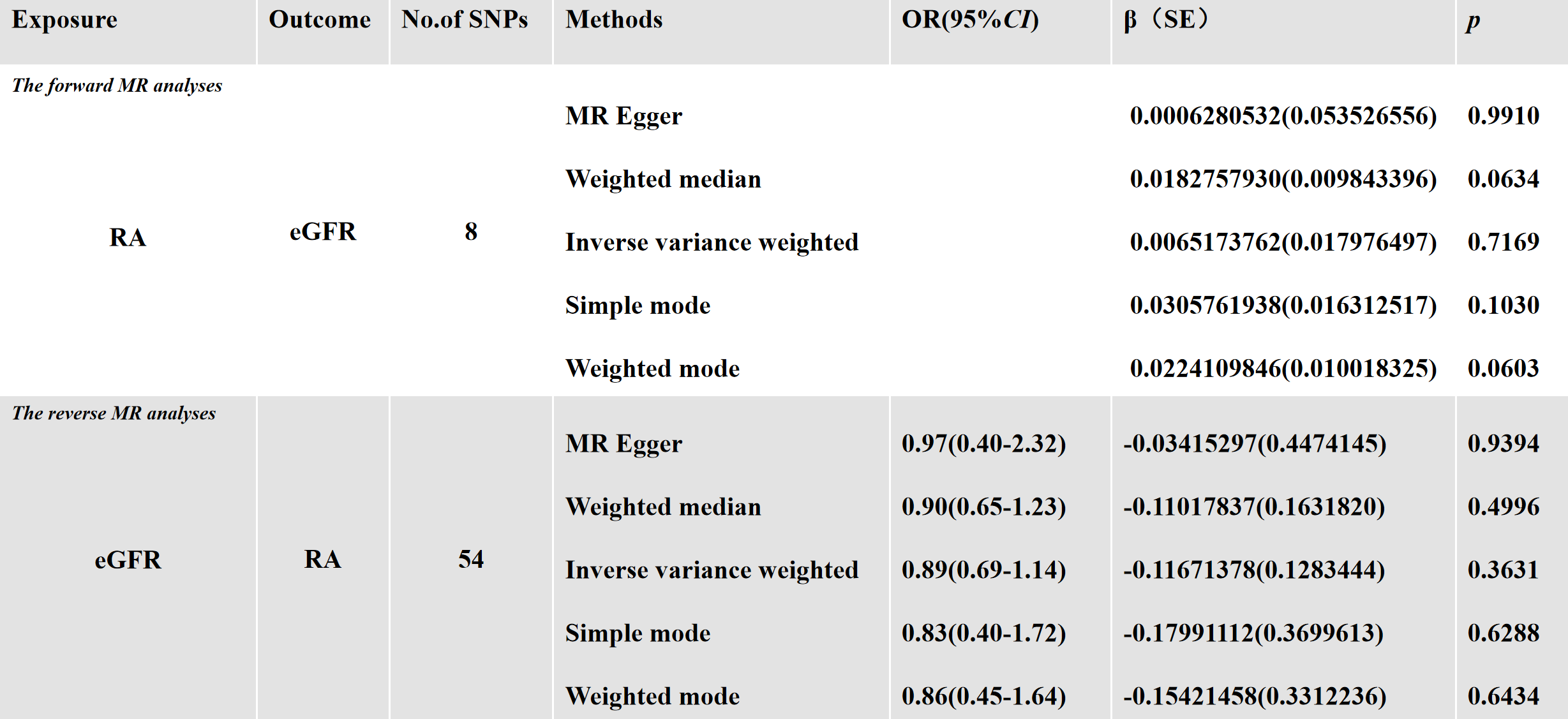
In this bidirectional two-sample MR analysis, there was no evidence to support a causal relationship between RA and kidney function in any direction. In previous studies on independence, most tended to believe that RA would lead to a decline in kidney function, which could be due to confounding factors or reverse causality [39]. However, we completed a reverse MR analysis in our study, which was able to eliminate the latter. LaTonya J Hickson et al. suggested that over time, RA patients are more likely to experience a decline in kidney function than healthy individuals, which may be related to cardiovascular disease [40]. SangHeonSuh et al. found that patients with RA had a higher incidence of end-stage renal disease than subjects without RA, and that the risk of end-stage renal disease(ESRD) was higher in relatively young individuals [41].MTX and some DMARDs, the most commonly used drug for the clinical treatment of RA, as mentioned earlier, has been found to have a risk of kidney damage in some studies [42–44], but other studies have shown that low-dose MTX (LD-MTX) is safe in mild to moderate CKD. Before the emergence of MTX and targeted biologics, the occurrence rate of CKD in RA patients is quite high, and most RA patients with CKD in recent years are concentrated in Asia, which may be due to the difference in drug selection of DMARDs in Asia and Western countries, which also indicates the great influence of drugs on the outcome.Daniel H Solomon et al. found in a randomized trial conducted in patients without rheumatic disease that the use of LD-MTX was associated with a mild to moderate increase in the risk of skin cancer and gastrointestinal, infectious, pulmonary, and hematological adverse events, while the risk of renal adverse events was decreased [45–46]. This may indicate that the use of MTX is a more potent confounding factor. Therefore, relevant factors have been filtered out before screening for appropriate SNPs, and the final result indicates that RA and kidney function are not related. Based on this, we can speculate that RA itself does cause kidney damage, but mesangial proliferative glomerulonephritis(MPGN) and membranous nephropathy(MN), which account for a relatively large proportion of renal lesions, have no significant damage to GFR.At the same time, the negative result of MR Analysis does not directly mean that RA and renal function have no causal relationship and are independent of each other.As mentioned above, MPGN is the most common in the course of RA disease, followed by amyloidosis and MN. As the disease is relatively mild, eGFR measured by blood creatinine level is normal in most RA patients with mesangial and membranous GN, and when amyloidosis occurs in patients' kidneys, it indicates that the lesion is more serious.Its typical manifestation is complicated by progressive renal failure [16], which must be accompanied by a decline in eGFR.It was found that eGFR decline, an outcome event, was not sensitive enough to expose RA.What's more,it is worth noting that eGFR is related to factors such as age and environment [47, 48], and environmental factors related to RA such as smoking, obesity, and gut microbiota have also been shown to have a clear correlation with eGFR [49–54]. We have reason to believe that the observation in most studies that RA patients often have a decline in kidney function should be attributed to the complex interactions between RA and various systems in the body and cannot be summarized by causal relationships.
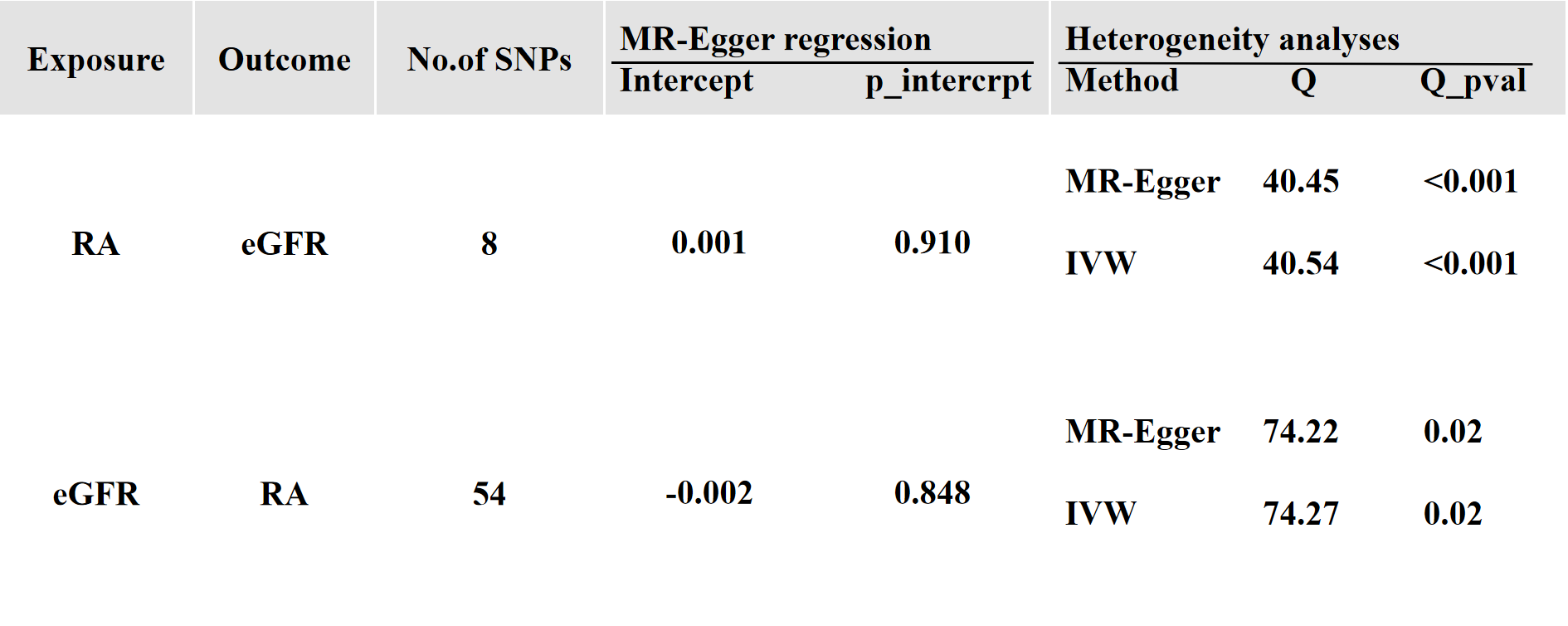
Although TSMR analysis was used and instrumental variables were rigorously screened, this study still has limitations, such as the unsatisfactory results of instrumental variables in heterogeneity testing. Although the rigorous screening and testing of SNPs made the results robust,but exposure and outcome were selected from the same database,bias may still be caused by a small number of genetic instruments, small sample size, or potential sample overlap between exposure and outcome. Secondly, using eGFR instead of kidney function.The indicator cannot fully represent kidney function. Because Scr and BUN based eGFR sensitivity is relatively low and is influenced by many non-GFR factors such as muscle mass, diet, age, etc.Moreover, factors such as race and genetics do have an impact on eGFR [55, 56]. This study only covered the East Asian population, and in the future, GWAS databases from Europe, Africa, and other regions should be included to more clearly understand the relationship between RA and kidney function.
If we want to further comprehensively study the relationship, human metabolic products such as uric acid and creatinine,serum cystatin C,β2-microglobulin ,wihch can be sensitive to the indicators of early renal damage,should be included, and previous studies have pointed out that the creatinine-cystatin C equation has unique advantages in measuring kidney function [57]. CysC is produced by nucleated cells in vivo, and circulatory CysC is only cleared by the kidney, which is an ideal indicator of GFR in patients with normal to moderately impaired renal function [58–59].Moreover, since GWAS were aggregated data, we could not conduct additional analysis, for example, taking RA patients' age and duration of disease or drugs used as exposure, and taking more refined metabolic indicators as outcome.The hope is that the current study can be refined when the data are more detailed.
{kind=link}
{kind=link}
{kind=link}
{kind=link}