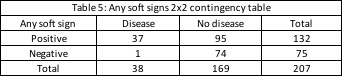
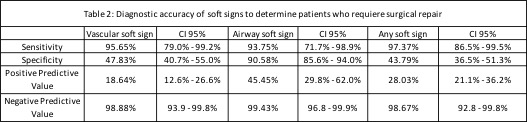
Our study’s main findings suggest that in settings with limited resources, patients with PNI and no vascular, airway or gastrointestinal soft sign can be safely managed with a conservative approach. These hold high negative predictive values in the absence of soft sings (NPV: 93% -99%). Our findings also demonstrate that adequate identification of soft signs represents a reasonable screening tool for patients with PNIs, as it shows high sensitivity (97.4%) [CI] [86.5% - 99.5%] in determining patients who require surgical repair. Many high-volume trauma centers are using the Selective Non-operative Management Approach (SNOM) (8). These works by determining the soft signs of vascular injury, airway injury and upper gastrointestinal tract lesion. SNOM help suspect vital structure lesions and to identify the need to carry out complementary studies (8). Similar to our results, the study of Inaba et al. with 453 patients at two Level 1 trauma centers demonstrate that using physical examination to triage patients into those with hard signs, soft signs, and no signs of vascular and aerodigestive tract injuries was highly effective at minimizing the need for invasive imaging and the rate of negative surgical exploration (17). Different studies validated the practice of SNOM as a safe an appropriate management strategy (8,18).
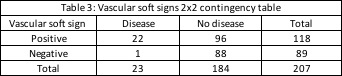
Identification of vascular soft signs evidenced high sensitivity (95.6%) [CI] [79% - 99.2%] and NPV (98.9%) [CI] [93.9% - 99.8%] in order to determine patients who require surgical repair. The possibility of requiring surgical repair if one does not present any vascular soft sign is low. While some authors advocate mandatory vascular imaging following PNIs according to mechanism or zone, many studies have demonstrated the reliability of physical examination alone to exclude clinically relevant vascular injuries (12, 19). The no zone approach has become more relevant as identification of soft signs hold higher value to identify lesions that require repair, regardless of the zone of the neck injured (18). A prospective observational study with 203 patients showed a negative predictive value (NPV) and specificity of 88.6%–95.5% and 90.7% respectively, for all signs and symptoms mandating angiography (19). Additionally, in a study conducted with 216 patients in Indiana the sensitivity and negative predictive value of physical examination for detecting vascular injuries requiring operative management were both 100% (12). Moreover, the research of Menawat et al. conducted with 110 patients evidenced that 42 patients were determined to have no vascular injury based on lack of any physical findings (20). According to our findings and evidence shown in literature it is safe to say that routine angiography may be unnecessary for patients with penetrating neck injuries and negative physical examination.
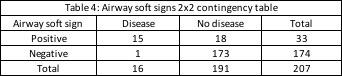
Taking into account soft signs of airway injury, our study showed a sensitivity of 93.8% [CI] [71.7% - 98.9%], a specificity of 90.6% [CI] [85.6% - 94%], and a NPV of 99.4% [CI] [96.8 – 99-9%] to diagnose airway injuries that required surgical repair. Patients presenting airway soft signs may be evaluated with bronchoscopy, esophagogram and esophagoscopy (12). Nevertheless, new technologies such as CTA have demonstrated to hold high diagnostic accuracy when compared to the vascular and airway diagnostic gold standards. Different studies showed nearly 100% sensitivity and specificity of CTA in detecting clinically significant vascular or aerodigestive injuries (17, 22-24).
As shown, any vascular or airway soft sign identified in patients should impact the management received. Different diagnostic studies (Arteriography, duplex of four vessels of the neck, bronchoscopy, esophagogram, esophagoscopy and more recently CTA) have shown high sensitivity and negative predictive values to determine injuries in patients with PNI (12,23). Although, we should bear in mind the significant resource implications associated with unnecessary utilization of diagnostic tools (17). In a resource-limited environment, unnecessary procedures may be interpreted as the loss of opportunity in the care of many patients, which is why the confirmation of the safety and accuracy of physical examination in patients with PNI represents a valuable strategy towards a simpler, more economic, accurate, and widely applicable method of determining the proper management of these patients (21).
A consensus regarding the management of penetrating neck injuries has been sought around the world. It is clear that immediate neck exploration is warranted in unstable patients with ‘‘hard signs’’ of neck injury after optimal airway has been obtained (16). In accordance to international literature, our study showed higher incidence of stab wounds than gunshot wounds as a result of interpersonal violence within city limits (7,8,18,20,21). Nevertheless, higher incidence of gunshot wounds is evidenced in scenarios of war and armed conflict. Additionally, according to literature there´s a higher prevalence of PNIs in men, and the most affected zone of the neck is usually zone II (18-21). However, the type of management of the PNI shouldn’t be determined by the mechanisms of assault or neck zone affected but by the signs and symptoms presented by the patient (4,7,12,19).
There are some limitations to this study that need to be emphasized. Primarily, this was an observational retrospective study. If we wish for there to be a future paradigm shift towards a SNOM approach in scenarios of low resources, a prospective study would be more appropriate. Also, a bigger sample size could help corroborate our results. Additionally, the hospital where the study was conducted did not have available CTA imaging. As different studies showed a nearly 100% accuracy in detecting vascular and aerodigestive injuries, it would have been important to count on this diagnostic tool as a gold standard.
{kind=link}
{kind=link}
{kind=link}
{kind=link}