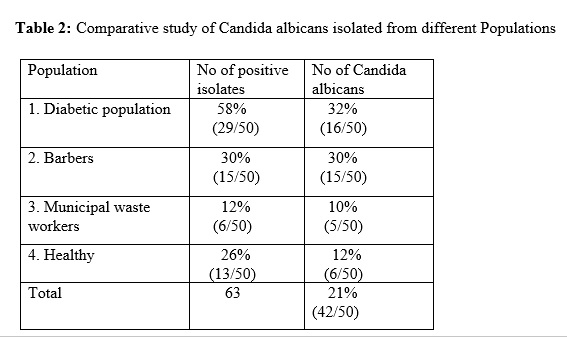
Research design: The cross sectional lab based study was carried out in microbiology laboratory of Central campus of Technology, Hattisar from June 2018 to November 2018. During the study 200 oral rinse samples were analyzed. All the work concerning this research was carried out in microbiology laboratory in Central Campus of Technology, TU, Hattisar, Dharan. The different oral rinse samples analyzed were from different potential risk population (50-barbers, 50-municipal waste workers, 50-diabetic and 50-healthy individuals).Ethical approval was obtained from Nepal Health Research Council, Kathmandu. The research participants were informed about the procedure of sample collection and the informed consent was obtained in written form. All the participants without oral lesions were included in the study. The Healthy population was selected by Nutritionist on basis of physical fitness, good oral hygiene whereas Diabetic population was selected on basis of blood glucose level obtained from their medical history. All the socio-demographic information like brushing habit, Gutkha chewing e.t.c was obtained from research participants through Schedule.
Inclusion criteria
Group I patients: In the inclusion criteria, 50- participant having DM without any other oral lesions with following criteria were included in the study. Participants who have not received antibiotic and corticosteroid therapy before 4 weeks were included in study.
- Random blood sugar (RBS) ≥200 mg/dl or
- Fasting blood sugar (FBS) >126 mg/dl.
Group II (Control group): 50-People who did not have DM or any other systemic illness, who were nutritionally fit, without any clinical signs of diseases, without any clinical medication were included as Healthy control.
Group III: It included 50-Barber population across the city.
Group IV: It included 50-Municipal waste worker of Dharan Sub metropolitan city.
Exclusion criteria
The people who never met above criteria were included under exclusion criteria
Sample collection
Ten ml of sterile saline were allowed to be rinsed for 1 minute and inoculated in a broader capped sterile container. The oral rinse sample for study were collected from the sample population and transported to microbiology laboratory maintaining cold chain .All the collected samples were labeled with participant's identification number. In case of delay, the sample was usually stored at 4°C in the refrigerator.
Processing of oral rinse in SDA
An aliquot of 50 microliter of oral rinse sample were inoculated in SDA (HiMedia, Mumbai, India) with chloramphenicol (0.05 g/l) and incubated at 37°C for 24-48 hours. Pure culture was identified by colony characteristics, grams staining. The number of colony was counted by Colony Counter and expressed as CFU/ml [14, 15].
Assessment of Candida colonization by Quantitative Enumeration
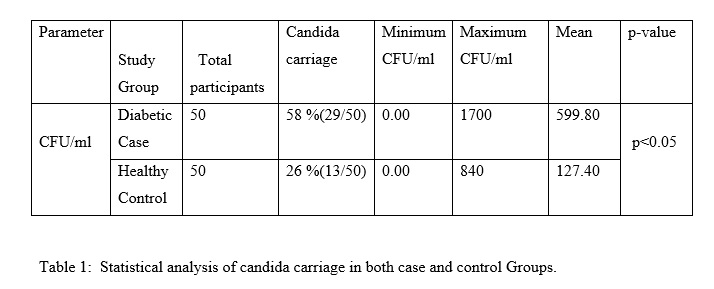
Number of colonies formed after incubation were counted by colony counter counted and multiplied with a factor of 20 to get the colonies in 1 ml of a subject’s sample [15].
Number of colonies contained in 50 μl of sample = n
Therefore the number of colonies in 1000 μl
(1 ml)
= n x 1000/50
= n x 20
Identification of Candida albicans
Germ tube and Chlamydospore formation was evaluated as described by Beheshti et al (1975) [16]. Germ tube test: The pure isolated colony of candida albicans was dispensed in 0.5 ml of serum and incubated at 37°C for 2 hours. After incubation the aliquote was taken in a clean slide and was observed under microscope for the formation of Germ-tube.
Chlamydospore formation test: The pure isolated colony of Candida that could form Chlamydospore in Corn Agar was identified as Candida albicans.
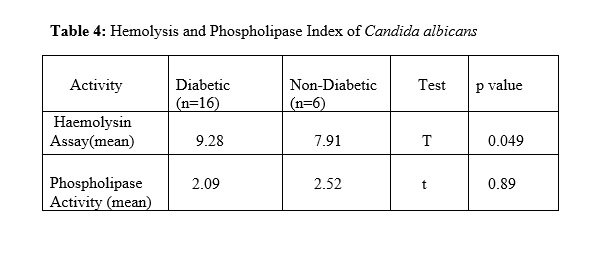
Hemolysin Assay
Haemolysin activity was evaluated according to Luo et al 2001[13]. Hemolysin production by Candida albicans was performed by inoculation overnight culture of yeast on Sugar-enriched sheep blood agar as described by Manns et al (1994) [13]. The Blood base agar media was prepared by adding 5-7 ml of fresh blood to Saboured Glucose Agar with 3% glucose. 10 µL of the yeast inoculum was placed at the centre of the plates. The plates were incubated at 37ºC in 5% CO2 for 48 hours. Hemolytic Index (Hz value) which represents the Hemolysin production is the ratio calculated by dividing the total diameter of the colony plus the translucent halo by the diameter of the colony.
Screening Candida albicans for production of phospholipase
The phospholipase test was done according to Samranayakae et al (1984) [17]. Egg yolk agar media was inoculated by 2 µL of the inoculum and allowed to dry at room temperature. The plates will be incubated at 37ºC for 3-4 days. 𝑃z will be measured by dividing the diameter of the colony by the sum of diameter of the colony and the zone.
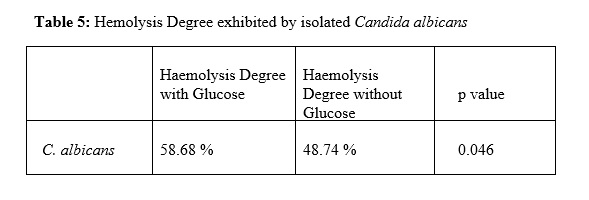
Screening impact of diabetes in hemolytic activity
The hemolytic activities were tested on Saboured dextrose Broth liquid media (SDB) containing 7% defibrinated human blood according to Malcok et al (2009) [12]. One was supplemented with 3% glucose and the other without glucose. Candida albicans culture was inoculated and incubated for 48 hrs. The hemolysis in the media was detected spectrophotometrically by measuring the amount of released hemoglobin and compared with a standard hemolysate which was prepared prior to testing. The degree of hemolysis (percentage value) by an individual strain was calculated according to the following formula below: (Absorbance of supernatant media at 540 nm/Absorbance of standard hemolysate at 540 nm X 100).
Biofilm Assays
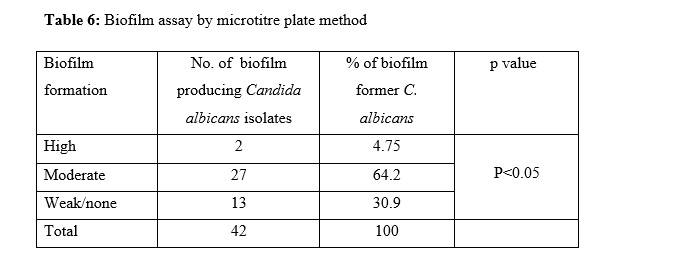
Microtitre plate method
The quantification of biofilm was performed according to Christensen et al (1985) [18]. In this method, 5 ml of overnight culture of Candida albicans was prepared. Then 100 microliter of diluted culture was inoculated in a sterile 96-well polystyrene well plates well containing TSB with glucose. The plate was incubated at 37ºC for 24 hours for biofilm production. The unbound cell was discarded and washes several times. 125 μl of 0.1 % crystal-violet solution was added and left for 10-15 mins incubation. The plate was washed and left inverted for dry. The quantitative Determination was performed by solubilizing the biofilm by adding 125 μl of 30% acetic acid to each well and incubated the plate for 10-15 mins at room temperature and was transferred to another microtitre plates and reading the absorbance at 570 nm by ELISA plate Reader. The interpretation of biofilm production was done according to the criteria of Stepanovic et al. (2007) [19].
|
Average OD
|
Value Biofilm production
|
|
≤ ODc / ODc < ~ ≤ 2x ODc
|
Non/weak
|
|
2x ODc < ~ ≤ 4x ODc
|
Moderate
|
|
> 4x ODc
|
Strong
|
Optical density cut-off value (ODc) = average OD of negative control + 3x standard deviation (SD) of negative control.
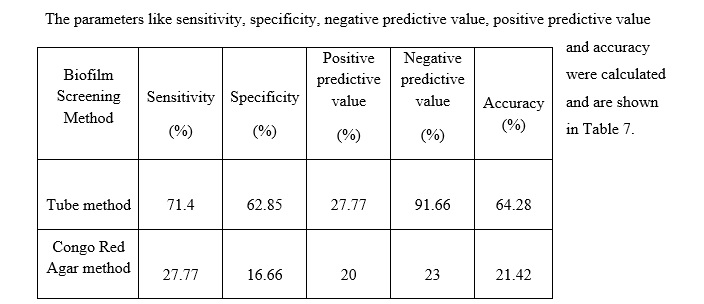
Tube method
A qualitative assessment of biofilm formation was done as described by Christensen et al (1985)[18]. The TSB glu (10 mL) was inoculated with a loop full of Candida albicans from overnight culture plates and incubated for 24 hours at 37°C. The tubes was decanted and washed with PBS (pH 7.2) and dried. Then the tubes were stained by 0.1% crystal violet. Stain was removed by deionized water. Tubes were then dried in inverted position for biofilm formation. Biofilm formation was considered positive when a visible film lined the wall and bottom of the tube. Ring formation at the liquid interface was not considered biofilm formation. An experiment was repeated for three times.
Congo red Agar Method (CRA)
The Candida albicans culture was streaked on surface of Congo Red Agar and incubated at 37ºC for 24-48 hours (Freeman et al 1989) [20]. Black coloured colonies with dry crystalline consistency interpreted as positive biofilm producing strains. Red coloured colonies- interpreted as negative for biofilm production.
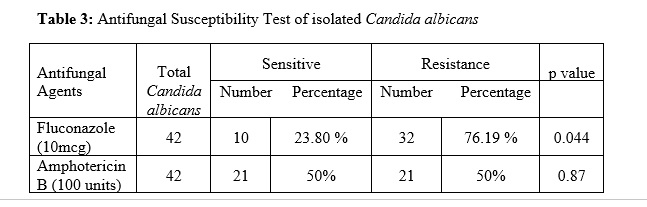
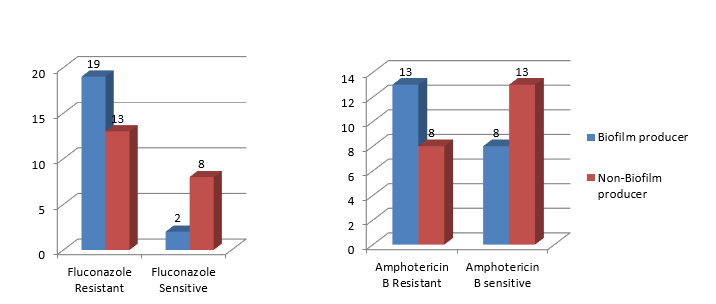
Antifungal Susceptibility Testing
All Candida albicans isolated from samples were subjected to in-vitro antifungal susceptibility test by Kirby-Bauer disc diffusion method as recommended by CLSI 2010 [21]. In this study the antifungal used were Amphotericin-B (100 Units) and fluconazole 10 (mcg) (Himedia, Mumbai India). In this study, the most preferred class of antifungal agents like polyenes and azoles was included; amphotericin-B (100 Units) and fluconazole (25 μg/mL.), (HiMedia, Mumbai, India) stored in at 4°C.Yeast inoculums were prepared by picking five distinct colonies of approximately one mm from each 24 hours old culture grew on Sabouraud Dextrose Agar (HiMedia, Mumbai, India) incubated at 35 ± 2°C. Colonies was suspended in 5 mL of sterile 0.85% Saline. Vortexed the resulting suspension and adjusted the turbidity to yield 1 × 106 - 5 × 106 cells/mL (i.e., 0.5 McFarland standard). A sterile cotton swab moistened with the inoculums suspension was used to apply to a 90 mm diameter plate containing Mueller-Hinton agar (HiMedia, Mumbai, India) supplemented with 2% glucose and 0.5 μg/mL methylene blue (GM-MH agar medium). The plates were allowed to dry for 5-15 minutes then after the disks were placed in the center of the agar plate. The plates were incubated for 18-24 hours at 37 ± 2°C and the slowly growing isolates will again read after 48 hours incubation. Zone sizes were measured in millimeters with Zone Scale (HiMedia, Mumbai, India); the zone diameter to the nearest point at which there was influential reduction in growth was taken into consideration. The organism was considered as resistant, intermediate or sensitive based on the standard interpretative chart according to CLSI standard (HiMedia Company, 2010).
Statistical Analysis
The data was analyzed using statistical Package for Social Sciences (SPSS) version 16.0. Mann Whitney U test was carried out to calculate CFU counts, Chi Square (χ2) were used for statistical analyses. The p value of equal or less than 0.05 was used for statistical significance.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}