Bacterial skin and skin structure infections, also known as skin and skin structure infections (SSSI), skin and soft tissue infections, and acute bacterial skin and skin structure infections (ABSSSI), impose a significant clinical and economic burden on the health care system (Seth et al. 2017). Previous studies revealed that, among nonfatal diseases, health burden, skin, and subcutaneous infections were 4th leading worldwide (Seth et al. 2017). Furthermore, It is anticipated that approximately 700 thousand people die each year because of anti-microbial resistance infections, and this figure will rise to 10 million by the year 2050 (O’Neill 2016).
Erysipelas, cellulitis, impetigo, folliculitis, and major cutaneous abscesses (furuncles and carbuncles) are the most common types of bacterial skin infection (Stulberg et al. 2002). Gram-positive bacteria (Staphylococcus aureus, Streptococcus pyogenes, Beta hemolytic streptococci, and enterococci) and gram-negative bacteria (Pseudomonas aeruginosa and Escherichia coli) are predominant species of bacterial skin infections (Summanen et al. 1995; Moet et al. 2007; Ray et al. 2013). Though Staphylococcus aureus and beta-hemolytic streptococci were the leading cause of SSTI (Ray et al. 2013), now Gram-negative organisms and mixed pathogens (both Gram-positive and Gram-negative bacteria) significantly caused acute skin infections (Ray et al. 2013; Lipsky et al. 2014; Zilberberg et al. 2009; McGinnis Emily et al. 2016). Antibiotic resistance to anti-infective agents has risen globally, predominantly among isolates of S. aureus, which shows resistance against methicillin (methicillin-resistant S. aureus MRSA) and other antibacterial drugs. (Loewen et al. 2017; Lee et al. 2017). Furthermore, skin infections due to MRSA isolates are also shown resistant to fluoroquinolones and macrolides (Maina et al. 2013; Baek et al. 2016). Increased resistance causes higher morbidity and costs (Pallin et al. 2008; Suaya et al. 2014).
According to World Health Organization (WHO), Antibiotic resistance is highly increasing worldwide. The efficiency of many antibiotics decreased may be due to bacterial multidrug-resistant genes, transposons, plasmids, chromosome, and its expressions. WHO has provided a list of antibiotic-resistant bacteria to guide researchers in discovering and develop new antibacterial agents against multidrug-resistant bacteria. Gram-negative MDR bacterial species, especially Pseudomonas aeruginosa and Enterobacteriaceae, is considered the most serious group (WHO 2017). In 2021, the World Health Organization considered antimicrobial resistance (AMR) as one of the top ten public health threats in global health (WHO 2021). Moreover, the Infectious Disease Society of America has also highlighted a small group of antibacterial resistance bacteria (Staphylococcus aureus, Klebsiella pneumonia, Enterococcus faecium, Acinetobacter baumanni, Pseudomonas aeruginosa, and Enterobacter) (Boucher et al. 2009), which shows resistance to many antibiotic drug classes and are a high priority for drug discovery. As problems in treating bacterial infections are increasing, the development of new antibiotics is more critical nowadays than ever.
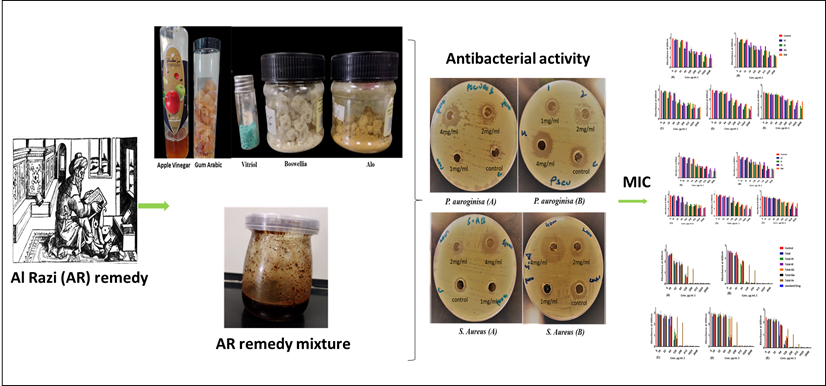
For thousands of years, natural products have been used in traditional medicine worldwide and introduced antibiotics and other modern drugs (Kafaru 1994). In developing countries, it is an easily available method to treat infections and other diseases; in some regions, around 80% of the population uses traditional medicine to fulfill their primary healthcare needs (Maroyi 2013). Plants used in traditional medicinal practices against infections have been found to inhibit the growth and virulence of various microbes (Ahmad and Beg 2001; Kumar et al. 2006; Bibi et al. 2011; Cioch et al. 2017). For this reason, researchers are increasingly focusing on herbal products, looking for new leads to develop better drugs against MDR microbe strains (Braga et al. 2005). Few famous Unani medicine (Perso-Arabic traditional medicine) books like the Canon of Medicine by Ibn Sina, Al Hawi by al Razi, Firdous al-Hikmah by al Tabari, and prophetic medicine by Ibn Qayyim. Al Jawziyya, describe impetigo as a dermatological disease. A remedy said to be effective even in severe cases was mentioned in them. The treatment seems promising, giving the properties of its ingredients. The mixture: “كندر، كبريت، صبر، زاج بالسواء صمغ درهمين و يطلى بالخل” “the same amount from Boswellia, aloe, and vitriol then add double quantity of gum Arabic, then add vinegar.”
Previous studies revealed antimicrobial activity of apple vinegar against different bacterial strains such as Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus pyogenes, Streptococcus pneumonia, Enterococcus faecalis, Pseudomonas aeruginosa, Pseudomonas fluorescens, Escherichia coli, Salmonella typhi, Klebsiella pneumonia, Proteus Vulgaris, Proteus mirabilis, Enterobacter aerogenes and Acinetobacter (Hindi 2013; Hindi et al. 2014). The Gum Arabic (GA) plant or Acacia gum was also reported for antibacterial, anti-inflammatory, antihypertensive, vasoconstrictor actions, antispasmodic activities, inhibitory effect against hepatitis virus, cytotoxic activities and antioxidant activity (Gilani et al. 1999; Malviya et al. 2011). In traditional Arabic and Asian medicine Boswellia sacra oleoresin (frankincense) has been using as antibacterial agent for at least 1000 years (Rashan et al. 2021). Aim of the present study was designed to evaluate the antibacterial potential of Ancient Al Razi (AR) Remedy against dermatological infections. To find out antibacterial activity of AR remedy we had tested full remedy, drop out batches and each ingredient of this remedy alone in water or in vinegar against five common skin infections bacterial strains; Staphylococcus aureus ATCC 25293, Staphylococcus aureus ATCC 29213, Streptococcus pyogenes ATCC 19615, MDR Pseudomonas aeruginosa ATCC 27853 and clinical strain of Pseudomonas aeruginosa NR_117678.1.
{kind=link}