In this study we have explored autoantibodies in relation to SSc-ILD and show that autoantibodies towards Ro52 are enriched in BAL fluid, and that the presence of these antibodies in serum is associated with progression of SSc-ILD.
Prior cross-sectional cohorts have evaluated the clinical significance of anti-Ro52 in patients with SSc. In these studies, the presence of anti-Ro52 was associated with the presence of ILD. To our knowledge, previous studies have not evaluated whether the presence of anti-Ro52 predicts progression of SSc-ILD, although one study demonstrated that anti-Ro52-positivity is associated with worse survival in patients with SSc (20). In other disease states, including mixed connective tissue disease (MCTD) (40) and idiopathic inflammatory myositis, the presence of anti-Ro52 is associated with progression of ILD (41). Moreover, in patients with antisynthetase syndrome, the presence of anti-Ro/SSA was more common in patients with severe ILD (42).
One longitudinal study evaluated whether the presence of anti-Ro (measured by immunodiffusion) was associated with lung function decline in patients with SSc, including both patients with and without ILD (19). However, the immunodiffusion method employed by this study only precipitates anti-Ro60, and not anti-Ro52 (43, 44). While Ro52 and Ro60 have historically been grouped together, they in fact have limited structural and functional homology with each other (45) and individually distinguish separate disease phenotypes (46). In this study we used ALBIA multiplexing technology, a method that accurately analyzes presence and semi-quantitative concentration of autoantibodies against Ro52 and Ro60 separately (46–48).
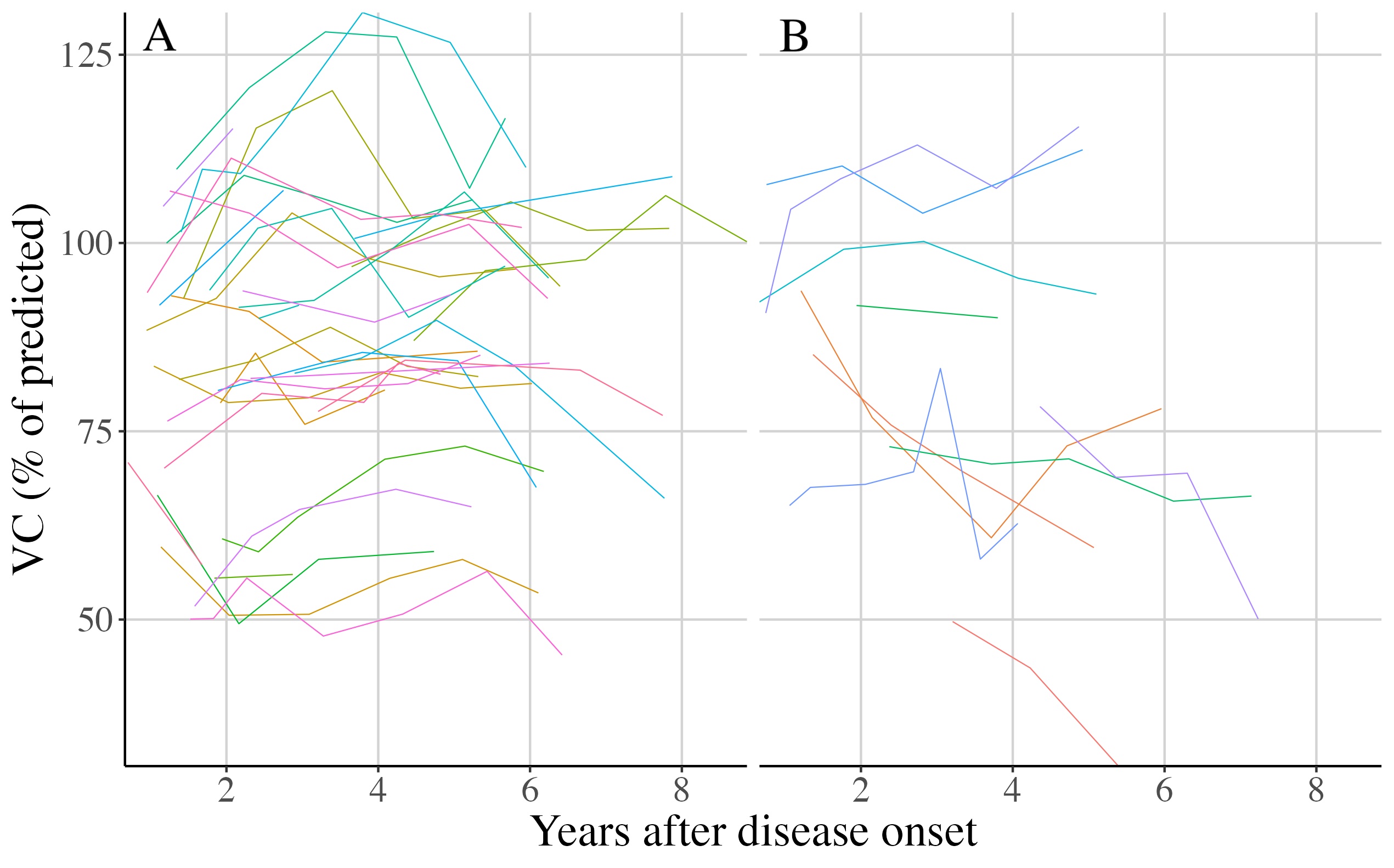
In addition to anti-Ro52 presence, we also explored the possible association between anti-Ro52 antibody levels and SSc-ILD progression (Fig. 4). Our results are in agreement with recent reports in antisynthetase syndrome were higher levels of anti-Ro52 are associated with more severe disease (49). Similar findings have recently been presented in congenital heart block and anti-Ro52, further raising the questions if the concentration of Ro52-antibodies may be of also clinical importance (50). Our results on anti-Scl70-levels are also in line with previous observations of an inverse relationship between anti-Scl-70 concentration and %VC (51).
Our study adds new perspective on the association between anti-Ro52 and lung fibrosis as we were able to demonstrate an accumulation of anti-Ro52 autoantibodies in the BAL fluid. This finding suggests a pathobiological link between the presence of anti-Ro52 antibody and the progression of ILD. Also, our BAL-results were carried out in patients with new-onset disease with relatively modest SSc-ILD. These findings are in line with previous reports suggesting that Ro-52 autoimmunity may precede development of ILD by several years (52). Of interest, ILD without co-existing rheumatic disease has been linked to an increased prevalence of anti-Ro52 seropositivity (53).
Few studies have investigated enrichment of autoantibodies in BAL fluid of SSc patients. One study from 2014 demonstrated that anti-citrullinated protein antibodies (ACPAs) are enriched in BAL fluid of ACPA-positive patients with rheumatoid arthritis, and that these patients also exhibit lung abnormalities during early stages of disease (24). In this study, it was hypothesized that early lung injury may initiate local molecular changes that generate immune responses in genetically susceptible individuals, subsequently causing systemic inflammatory disease. This hypothesis is of interest also to the SSc population considering our knowledge of inhaled environmental agents as a risk factor for SSc development (54, 55). Taken together, the results of the present study raise the question if autoimmunity against Ro52 is initiated locally in the lungs of anti-Ro52 positive patients that develop SSc-ILD.
In our exploratory analysis, we demonstrated that Ro52 is naturally present in both healthy peripheral lung tissue and fibrotic peripheral lung tissue, and can be localized to M2 alveolar macrophages. M2 macrophages are involved in wound healing, and M2 macrophages are reported to be increased in both the skin and the peripheral blood of patients with SSc (56, 57). Ro52 belongs to the tripartite motif protein family, which regulates the innate immune response including the antiviral immune response (23). Ro52 functions as an E3 ubiquitin ligase, tagging proteins for proteasome degradation by binding to the Fc-region of immunoglobulins, that is in turn bound to the target protein on its antigen-target site (23, 48). It is hypothesized that this property mediates an antiviral response that both degrades pathogens and regulates inflammatory mediators, such as the interferon regulatory factor (IRF) family (48, 58, 59). Experimental studies have shown that Ro52 may regulate the production of autoantibodies and that inhibition of this antigen may result in progression of autoimmunity (60).
Limitations of this exploratory study include the number of patients included. While statistically significant, the results we present in this study need to be replicated and validated in a large and independent cohort. Another limitation of the study is that we limited the number of covariates in our statistical model to anti-Ro52, anti-Scl-70, disease type, sex, and immunomodulator use, and in doing so, may have failed to include other predictors of lung function decline in the model. It is possible that the predictive power of anti-Ro52 may be mediated through some other predictors not included in our analysis. In addition, this study does not account for interaction effects between overlapping SSc-specific autoantibodies, or presence of anti-Ro60 autoantibodies. Another possible limitation is that the algorithm for determination of autoantibody levels using the proprietary FIDIS Theradiag software may underestimate very high antibody levels and thus overestimate the enrichment in BAL fluid. For that reason, and for follow-up studies, the Uppsala laboratory is currently developing new in-house algorithms for the comparison of autoantibody levels measured with ALBIA in different body compartments.
A strength of the study is its longitudinal design. Cross-sectional or survival analysis study designs are inadequate for drawing inferences about future ILD course (61, 62). Another strength of the present study is that all PFTs were made at the same center.
If validated, our results may have clinical implications for the future assessment and management of SSc-ILD. In comparison to several previously presented biomarkers of progressive SSc-ILD, such as KL-6, CCL2, CCL18, and CXCL4, assessment of anti-Ro52 autoantibodies is a routine analysis at rheumatological centers (63). Analysis of anti-Ro52 therefore has potential to be easily incorporated in the clinical risk stratification of SSc-ILD. (64).

{kind=link}