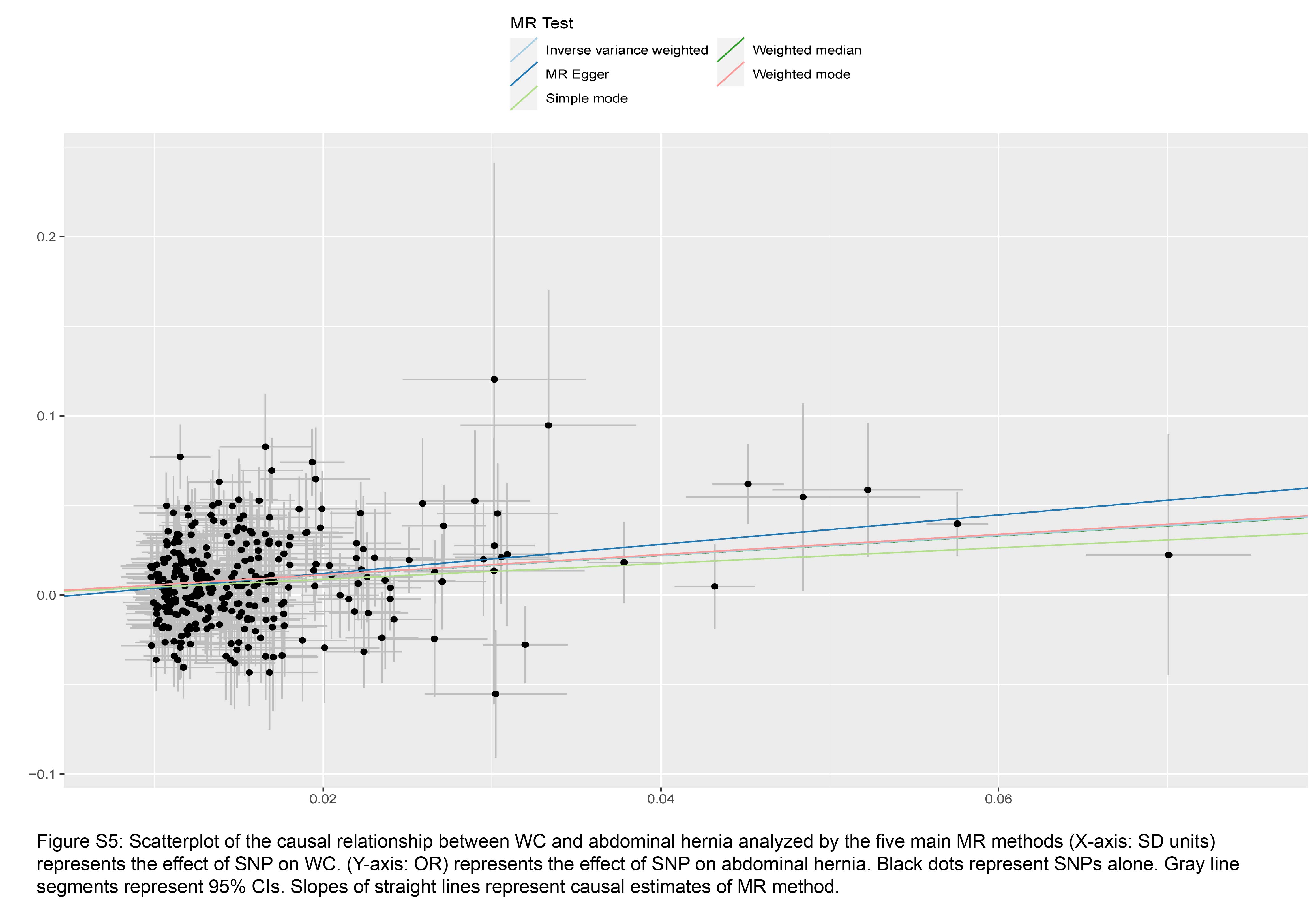
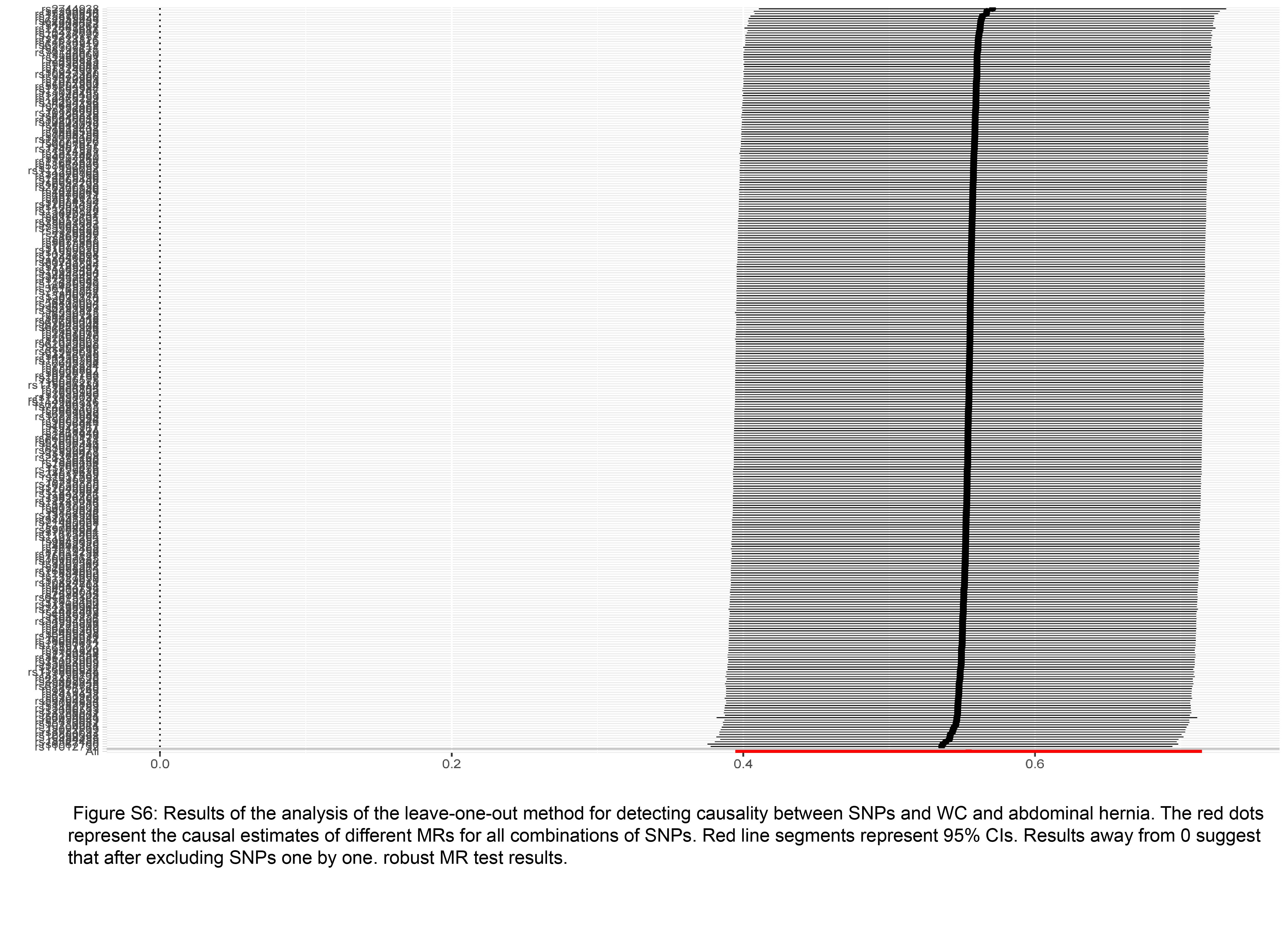
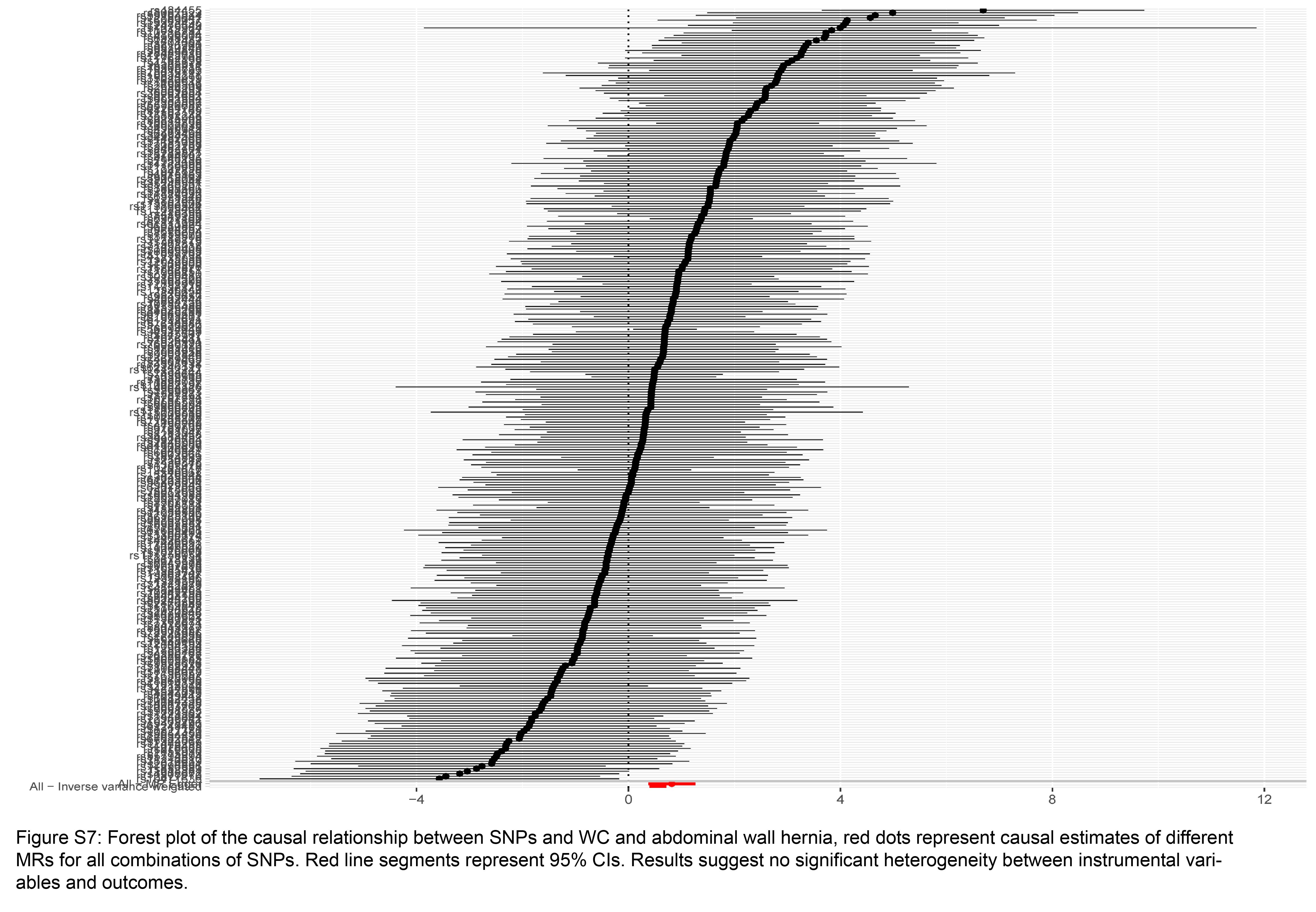
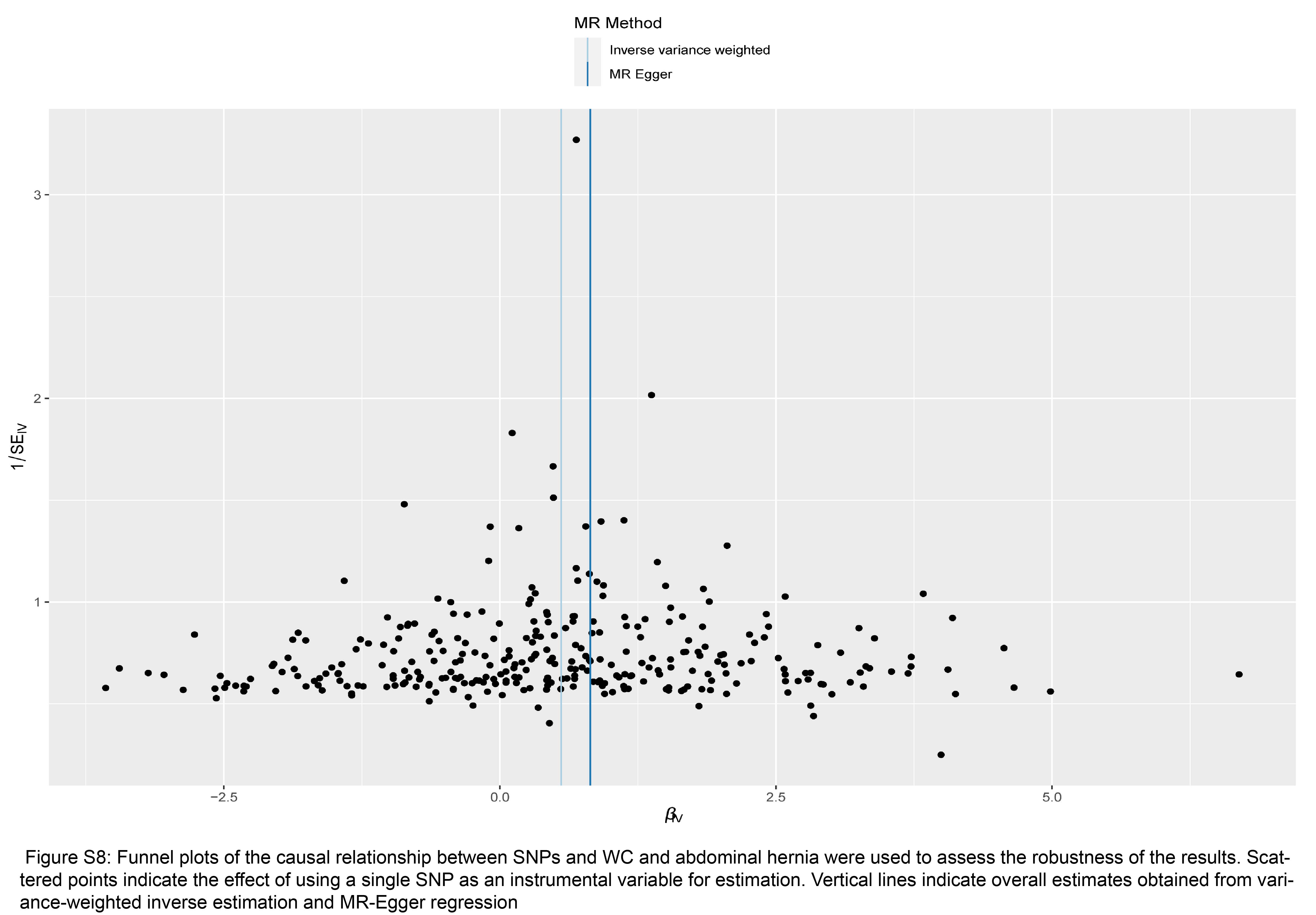
Our study results support that there is a causal relationship between obesity and AH. BMI, WC and BFP are commonly used to quantify obesity, and we found genetic evidence for the association of BMI, WC and BFP with AH by selecting the above three indicators as exposure factors for genetic phenotypes instead of obesity. Our results found that the risk of AH increased by 56% for each SD increase in genetically determined BMI, 55% for each SD increase in genetically determined WC, and 60% for each SD increase in genetically determined BFP. the risk of AH increased with increasing BMI, WC and BFP. The risk of AH increased with increasing BMI, WC and BFP. Indirectly, the risk of AH was shown to be higher in obese individuals.
Similar to our findings, several observational studies have described an increased risk of AH as well as an increased risk of postoperative complications associated with obesity [1, 2]. In contrast, significant weight loss in obese individuals can reduce the tension and complexity of repairing large abdominal defects. This allows the surgeon to avoid extensive tissue pulling activities and reduces postoperative tension at the closure, reducing wound complications [14]. Obesity increases abdominal pressure and the consequent abnormalities in connective tissue metabolism may be a relevant mechanism for abdominal wall hernia formation. Previous studies have shown that plasma Matrix metalloproteinases − 2 (MMP-2) and MMP-9 concentrations and activity are elevated in obese patients, and although MMP activity is essential for normal wound healing, MMPs regulate wound healing by degrading collagen, laminin, proteoglycan, elastin, and fibronectin in the ECM and promote epidermal cell migration during re-epithelialization [15]. However, excessive MMP production and disruption of the MMP to tissue metalloproteinase inhibitor ratio can lead to matrix disruption and abnormal healing [16, 17], This may be the pathophysiological mechanism by which obesity increases postoperative complications in AH.
It is well known that obesity is usually a lifestyle-induced disease with a genetic component that can be changed and controlled through diet and exercise [18]. Our study confirmed that as BMI, WC and BFP increased, the risk of AH increased. Therefore, weight loss may be beneficial in reducing the prevalence of AH and thus the associated medical expenses. Our study is useful for medical professionals to provide advice on weight management in obese patients, and maintaining a healthy weight may reduce the risk of AH.
Of course, our study has limitations. First, our study population was European and there may be limitations to generalize to other populations. In addition, our study does not describe how obese patients contribute to the development of AH. However, our findings support a causal relationship between obesity and AH, and as the risk of AH increases with increasing BMI, WC and BFP, it is still reasonable to recommend obese individuals to lose weight and maintain a healthy weight for the purpose of preventing AH.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}