Associations between TRs and survival in HCC patients
The results outlined below suggested that the expression of THRA was not associated with the survival rate in HCC patients, while low expression of THRB in tumor tissues was considerably associated with poor overall survival (Log rank P = 0.0121, Figure 1E) and disease-specific survival (Log rank P = 0.0191, Figure 1I). The subgroup analysis of THRB revealed that the downregulation of THRB in tumor tissue was a risk factor for 1-year (Log rank P = 0.0173, HR = 1.952 (1.139-3.346), Figure 1F), 3-year (Log rank P = 0.0045, HR = 3.477 (1.783-2.660), Figure 1G), and 5-year (Log rank P = 0.0032, HR = 1.752 (1.206-2.546), Figure 1H) OS in HCC patients.
Since THRB was closely associated with the survival outcomes of HCC patients, we further performed its subgroup survival analyses. As shown in Figure 2, in HCC patients with neoplasm histologic Grade 3-4, low expression of THRB was significantly associated with poor OS (HR = 2.220(1.224-4.025), Log rank P = 0.0088, Figure 2B), while no differences were found in HCC cases with Grade 1-2 (HR = 1.580(0.9919-2.517) Log rank P > 0.05, Figure 2A). Also, THRB under-expression was significantly contributed to poor OS in HCC patients with stage I-II (HR = 1.853(1.139-3.015), Log rank P = 0.0141, Figure 2C) and stage III-IV (HR = 2.193(1.167-4.108), Log rank P = 0.0064, Figure 2D). In the patients with Child-Pugh grade A, the downregulation of THRB was significantly led to poor OS (HR = 1.986(1.163-3.391), Log rank P = 0.0126, Figure 2E), but no significance was found in the cases with Child-Pugh grade B-C (HR = 0.9676(0.2694-3.595), Log rank P = 0.9602, Figure 2F).
Additionally, we performed a subgroup survival analysis based on the patients’ basic clinical information. As shown in Figure 3, downregulation of THRB was associated with poorer survival in males (HR = 2.429, Log rank P = 0.0002, Figure 3A) and Asian patients (HR = 2.547, Log rank P = 0.0038, Figure 3D), while no significant differences were found in females (HR = 0.9367, Log rank P = 0.8202, Figure 3B), and White patients (HR = 1.410, Log rank P = 0.1496, Figure 3C). The downregulation of THRB was risk factor both in the groups with and without alcohol consumption (HR = 2.062, Log rank P = 0.0234 and HR = 1.684, Log rank P = 0. 0199, respectively, Figure 3E-F).
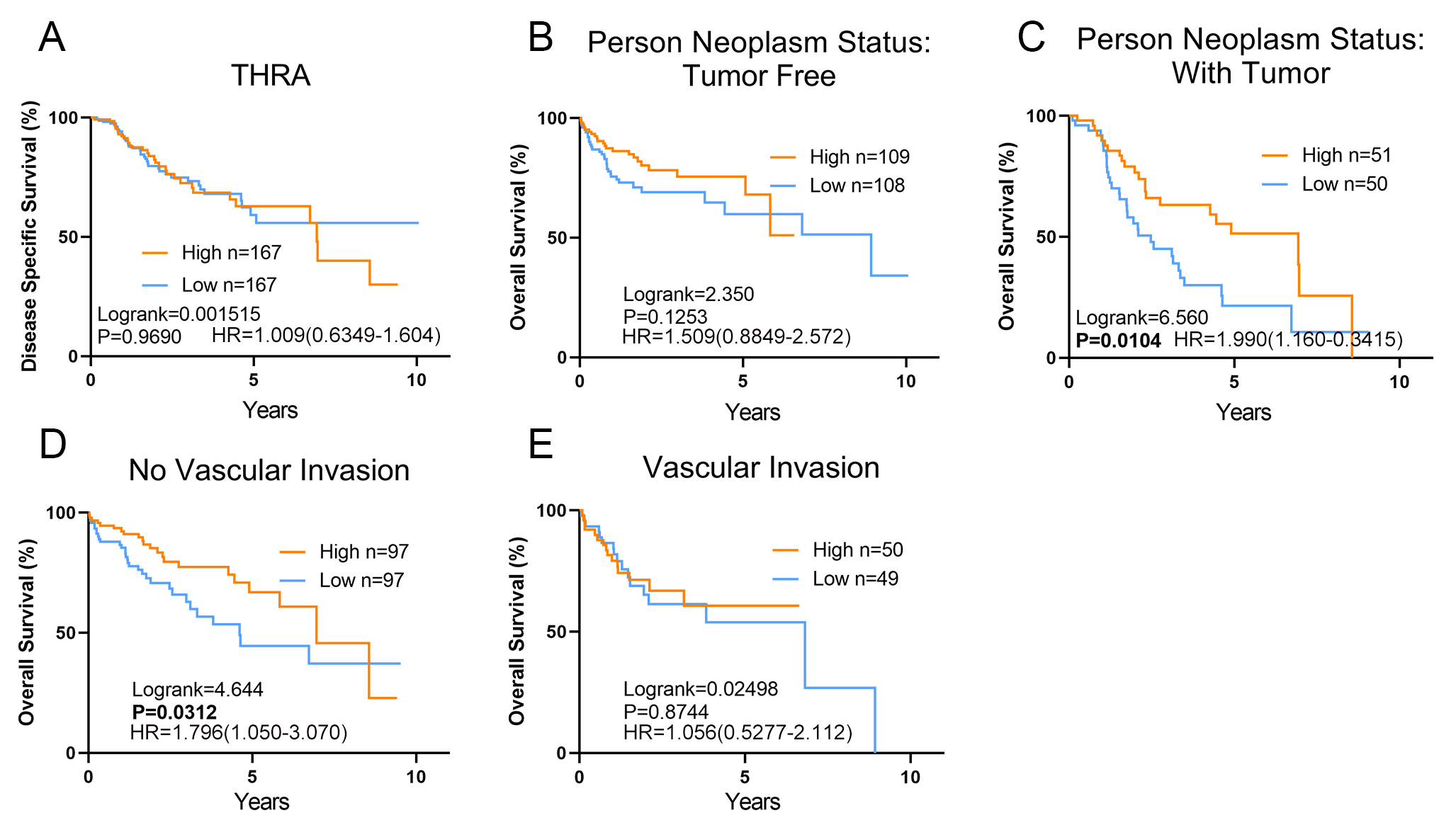
Moreover, we performed an exploratory subgroup survival analysis for THRB by the different clinical and biochemical parameters, including AFP level, person neoplasm status, vascular invasion, and liver fibrosis. As shown in Figure 3, low THRB levels significantly contributed to worse OS in HCC patients with hepatitis virus infection (Log rank P = 0.0012 HR = 2.865(1.537-5.342), Figure 3E). And downregulation of THRB was associated with poorer survival in the patients with high AFP level and no liver fibrosis (HR = 2.284(1.072-4.865), Log rank P = 0.0344 and HR = 2.907(1.347-6.273), log rank P = 0. 0107, respectively, Figure 3J-K), while no significant differences were found in low AFP level and liver fibrosis patients (HR = 1.385(0.7989-2.400), Log rank P = 0.2442 and HR = 1.476(0.7553-2.921), log rank P = 0. 2656, respectively, Figure 3I, L). Low THRB levels also significantly contributed to worse OS in HCC patients with tumor and no vascular invasion (HR = 1.990(1.160-3.415), Log rank P = 0.0104 and HR = 1.796(1.050-3.070), Log rank P = 0. 00312, respectively, Figure S1 C-D).
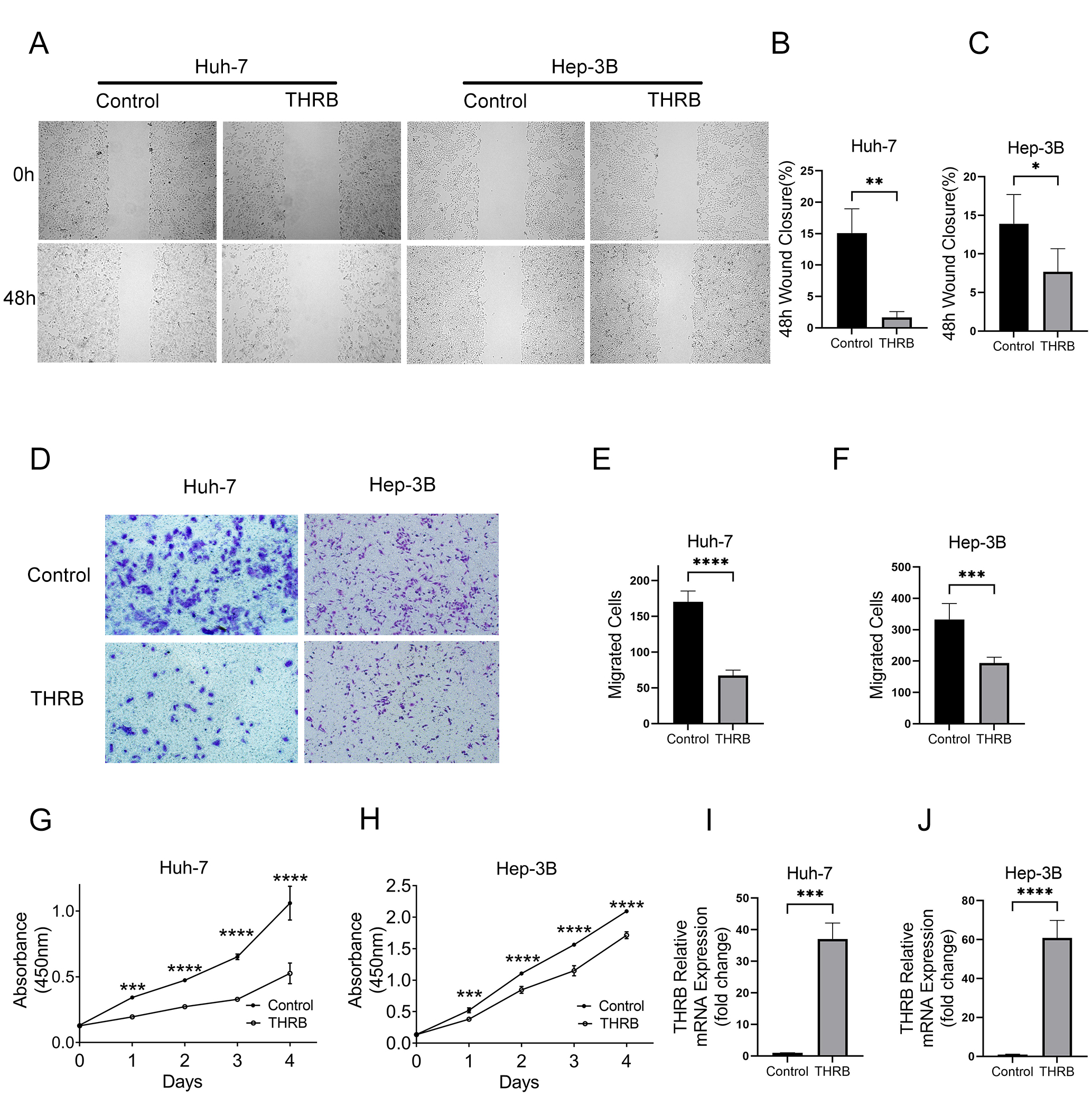
To further explore the roles of THRB in HCC cells. Huh-7 and Hep-3B cells were transfected with THRB and control plasmid. The overexpression efficiency was confirmed via qRT-PCT analysis (Fig. S2 I-J). Wound closure, Transwell and CCK-8 assays suggested that THRB could suppress the proliferation and migration of HCC cells (Fig. S2 A-H).
TRs expression comparison
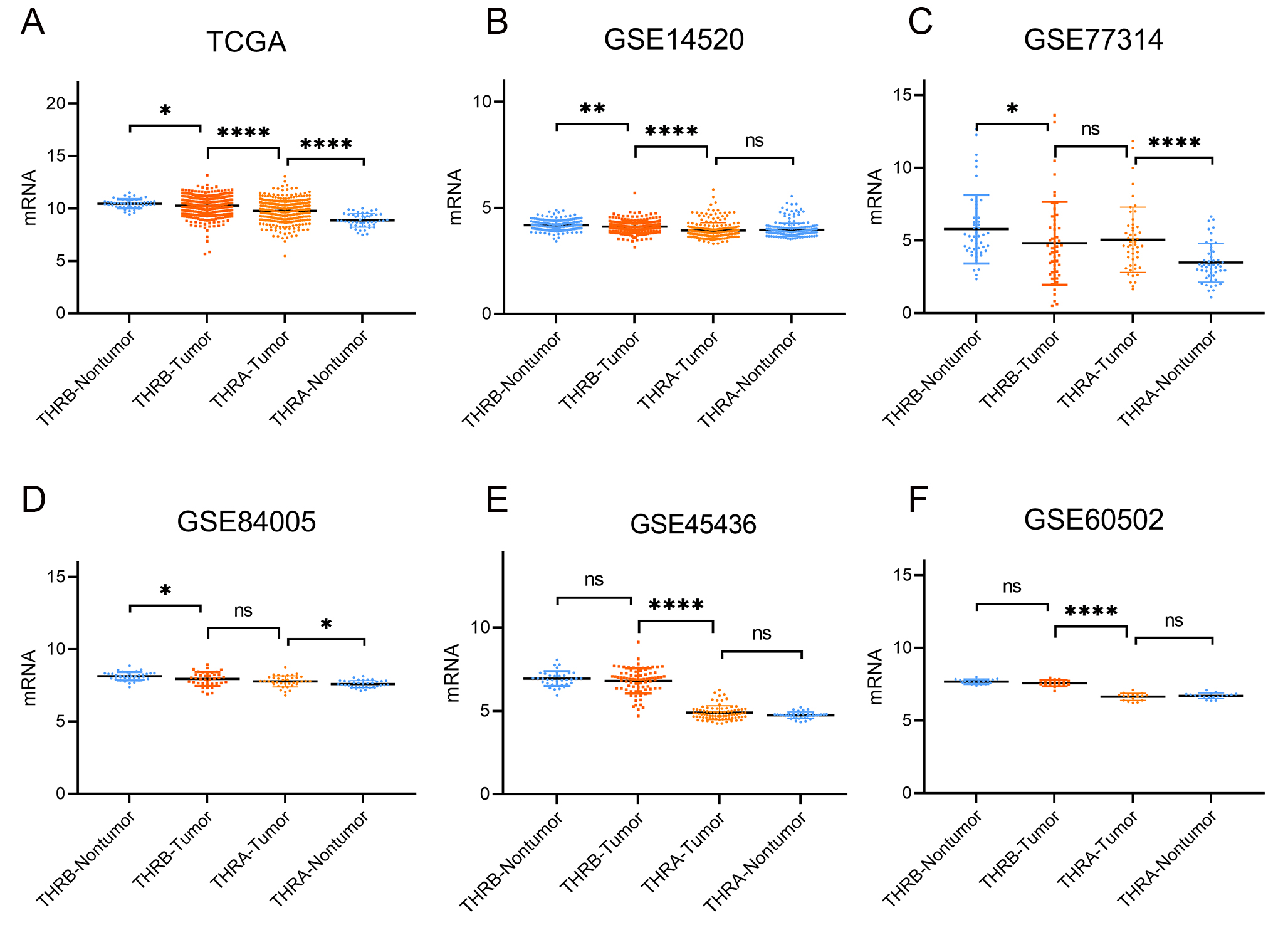
The details of GEO series involved in this study were presented in Table 1. As illustrated in Figure 4, the expression of THRB in tumor samples was significantly lower than non-tumor samples in TCGA, GSE14520, GSE77314 and GES84005 datasets (all P < 0.01), while no significant changes in GSE 60502 and GSE 45436 datasets. We also found the expression of THRA in tumor samples was significantly increased in TCGA, GSE 77314 and GSE 84005 datasets, while no significant increase was observed in GSE 14520, GSE 60502 and GSE 45436 datasets. We also performed the comparation between THRB and THRA, the THRB expression was significantly higher than THRA expression in tumor samples in TCGA, GSE 14520, GSE 60502 and GES 45436 datasets, while no significant change in GSE 77341 and GSE 84005(Figure S3).
Because the expression of THRB was not significantly decreased in all these datasets and samples, we further calculated the proportion of THRB down-regulated patients with paired samples based on 4 GEO series. As shown in Table 2, a total of 339 HCC patients, we found 193 patients (56.93%) with reduced expression of THRB (log2 fold-change < 0), 42 patients (12.39%) with log2 fold-change < -0.5 and 11 patients (3.24%) with log2 fold-change < -1.
|
Table 2. The percentage of THRB down-regulated patients
|
|
GEO series
|
Pairs
|
THRB mRNA Fold Change(log2)
|
|
Under-Expression Percentage
|
|
≤0
|
≤ -0.5
|
≤ -1
|
|
≤ -0.5
|
Total
|
|
GSE14520
|
233
|
145
|
21
|
4
|
|
9.01%
|
62.23%
|
|
GSE77314
|
50
|
14
|
9
|
5
|
|
18.00%
|
28.00%
|
|
GSE84005
|
38
|
22
|
11
|
2
|
|
28.95%
|
57.89%
|
|
GSE60502
|
18
|
12
|
1
|
0
|
|
5.56%
|
66.67%
|
|
Total
|
339
|
193
|
42
|
11
|
|
12.39%
|
56.93%
|
Association between THRB and clinicopathological features in HCC patients
As delineated in Table 3, there are more cases with Neoplasm histologic grade 3-4 in the THRB low-expression group (43.27% vs. 30.77%, P = 0.023) than those in the THRB high group. However, age, gender, race, family history of cancer, alcohol consumption, hepatic virus infection, tumor stage, Child-Pudge classification, AFP, fibrosis, adjacent hepatic tissue inflammation and vascular invasion were not significantly different in THRB expression (P> 0.05).
|
Table 3. Characteristics of HCC patients between THRB high and low groups
|
|
Variables
|
|
High (n=179)
|
Low (n=178)
|
P
|
|
Age
|
< 45 (n=37)
|
19
|
18
|
0.72
|
|
> 60 (n=189)
|
91
|
98
|
|
|
45-60 (n=131)
|
69
|
62
|
|
|
Gender
|
Female(n=117)
|
62
|
55
|
0.522
|
|
Male(n=240)
|
117
|
123
|
|
|
Race
|
White(n=172)
|
0
|
1
|
0.564
|
|
Asian(n=152)
|
72
|
80
|
|
|
Black or African American(n=16)
|
9
|
7
|
|
|
American Indian or Alaska Native(n=1)
|
90
|
82
|
|
|
Family History of Cancer
|
NO(n=199)
|
92
|
107
|
0.089
|
|
YES(n=103)
|
59
|
44
|
|
|
Hepatocarcinoma Risk Factors
|
Alcohol-consumption(n=110)
|
50
|
60
|
0.308
|
|
None(n=211)
|
108
|
103
|
|
|
Other(n=12)
|
8
|
4
|
|
|
Hepatitis Virus Infection
|
Infection(n=154)
|
75
|
79
|
0.487
|
|
None(n=167)
|
83
|
84
|
|
|
Other(n=12)
|
8
|
4
|
|
|
Liver Fibrosis Ishak Score Category
|
0-NoFibrosis(n=71)
|
40
|
31
|
0.312
|
|
1,2-PortalFibrosis(n=28)
|
12
|
16
|
|
|
3,4-FibrousSpeta(n=27)
|
11
|
16
|
|
|
5-Nodular Formation and Incomplete Cirrhosis(n=8)
|
2
|
6
|
|
|
6-Established Cirrhosis(n=65)
|
34
|
31
|
|
|
Adjacent Hepatic Tissue Inflammation Type
|
Mild(n=94)
|
50
|
44
|
0.32
|
|
None(n=112)
|
68
|
44
|
|
|
Severe(n=16)
|
7
|
9
|
|
|
AJCC Stage
|
Stage I-II(n=247)
|
126
|
121
|
0.205
|
|
Stage III-IV(n=83)
|
35
|
48
|
|
|
Neoplasm Histologic Grade
|
G 1-2(n=214)
|
117
|
97
|
0.023
|
|
G 3-4(n=126)
|
52
|
74
|
|
|
Child-Pugh Classification
|
A(n=206)
|
104
|
102
|
0.175
|
|
B-C(n=22)
|
15
|
7
|
|
|
AFP
|
< 100 ng/ml(n=181)
|
94
|
87
|
0.378
|
|
> 100 ng/ml(n=84)
|
38
|
46
|
|
|
Vascular Invasion
|
Macro(n=14)
|
9
|
5
|
0.369
|
|
Micro(n=88)
|
40
|
48
|
|
|
None(n=195)
|
100
|
95
|
|
PPI and KEGG/GO biological process enrichment
The results of PPI analysis are shown in Figure 5. 8 hub genes including PIK3R1, KAT2B, NRIP1, EP300, CREBBP, MED13, NCOA2 and JMJD1C were interacted with THRB.
The KEGG pathway enrichment of THRB interactive genes showed that peroxisome, valine, leucine and isoleucine degradation, beta-Alanine metabolism, protein processing in endoplasmic reticulum, etc. were the most enriched pathways (Figure 5A). Additionally, GO analysis results showed that THRB-related genes were significantly enriched in the small molecule catabolic process, proteasomal protein catabolic process, organic acid catabolic process, fatty acid catabolic process, etc. at BP levels, mitochondrial matrix, cell leading edge, endosome membrane, peroxisome, etc. at CC levels and coenzyme binding, transcription coactivator activity and ubiquitin-like protein binding at MF levels (Figure 5 B-E).
The correlation between THRB and tumor immune infiltrating cells
The potential correlation of THRB and tumor immune cells (B cells, CD4+ T cells, CD8+ T cells, neutrophils, macrophages, and dendritic cells) was estimated based on TCGA data. Interestingly, neutrophils exhibited the highest correlation with THRB, highlighting the key role of THRB associated with neutrophils in tumor immune infiltrating cells as shown in Figure 6 A.
We further performed the Kaplan–Meier analysis to compare the overall survival between high and low levels of THRB expression with different immune cell infiltration. The results indicated that high immune infiltration status of neutrophil with different THRB expression achieved a worse prognosis than with low immune infiltration status(Figure 6B). Low THRB expression with high immune infiltration status of CD4+ Th2 and Myeloid derived suppressor cells were also associated with worse prognosis than that was in low immune infiltration group (Figure 6C, D), while with high immune infiltration status of CD4+ memory resting cells was associated with better prognosis(Figure 6E). And then, high THRB expression with high immune infiltration status of macrophage and M2 were also associated with worse prognosis than that was in low immune infiltration group (Figure 6F, G).
{kind=link}
{kind=link}
{kind=link}