This study is the first real-world data analysis of the efficacy of nivolumab, pembrolizumab, and atezolizumab, approved by the FDA for the treatment of advanced NSCLC. These drugs are widely used in the clinical practice. To the best of our knowledge, the efficacy of nivolumab, pembrolizumab, and atezolizumab monotherapies has never been directly compared in older patients in a real-world setting.
This study showed a lower ORR but a similar median OS compared to previously published RCTs (ORR: 4.3–22%; overall, 10.6%; DCR: 30.0–59.2%; overall, 46.7%) (Table 4). Age-related decline in the immune system, known as “immunosenescence,” may affect immune checkpoint suppression activity in older patients [19, 20]. In addition, many comorbidities may contribute to death from causes other than lung cancer in older adults [21, 22]. Notably, several real-world data on older patients have shown similar results. However, it is unreasonable to compare the efficacy of immunotherapy between the present study and the existing RCTs based on age. For an accurate comparison, many other parameters, such as tumor histology, PD-L1 score, treatment regimen, and line of therapy, must be corrected. Therefore, this study aimed to compare and analyze the efficacy and OS within the study cohort rather than directly comparing it with existing RCTs.
Table 4
Characteristics and outcomes of the pivotal randomized clinical trials and the present study
| Study | Treatment | Line | Histology % | Patients n | Age, Median (range) | ECOG ≥ 2 n (%) | PD-L1 Score (%) | PFS (months) | OS (months) | ORR (%) |
| KEYNOTE-010 | Pembro | ≥ 2 | Sq: 22 Non-sq: 70 Other: 3 | 344 | 63 (56–69) | 3 (1) | ≥ 50 | 3.9 | 14.9 | 21.2 |
| KEYNOTE-024 | Pembro | 1 | Sq: 18.8 Non-sq: 81.2 | 154 | 65 (33–90) | 0 | ≥ 50 | 10.3 | 30 | 20.7 |
| KEYNOTE-042 [17] | Pembro | 1 | Sq: 38 Non-sq: 62 | 637 | 63 (57–69) | 0 | ≥ 1 | 7.1 | 20 | 27.3 |
| CheckMate 017 | Nivo | ≥ 2 | Squamous | 135 | 62 (39–85) | 2 (1.5) | ≥ 10 | 3.5 | 9.2 | 20 |
| CheckMate 057 | Nivo | ≥ 2 | Non-sq | 292 | 61 (37–84) | 0 | ≥ 10 | 2.3 | 12.2 | 19 |
| OAK | Atezo | ≥ 2 | Sq: 26 Non-sq: 74 | 425 | 63 (33–82) | 0 | All-comer | 2.8 | 13.8 | 14 |
| IMpower110 [18] | Atezo | 1 | Sq: 25 Non-sq: 75 | 107 | 64 (33–79) | 0 | ≥ 50 or (IC ≥ 10) | 8.1 | 20 | 40.2 |
| Current study | Overall | ≥ 1 | Sq: 50 Non-Sq: 50 | 180 | 76 (74–78) | 7 (3.9) | All-comer | nr | 10 | 10.6 |
| Pembro Nivo Atezo | | | 49 61 70 | 75 (74–78) 76 (74–78) 76 (74–78) | 3 (6.1) 1 (1.6) 3 (4.3) | | | 12.6 8.4 7.7 | 22.4 8.2 4.3 |
Abbreviations: ECOG, Eastern Cooperative Oncology Group; PFS, progression-free survival; OS, overall survival; DCR, disease control rate; nr, not reported; Pembro, pembrolizumab; Nivo, nivolumab; Atezo, atezolizumab; Sq, squamous; Non-sq, non-squamous
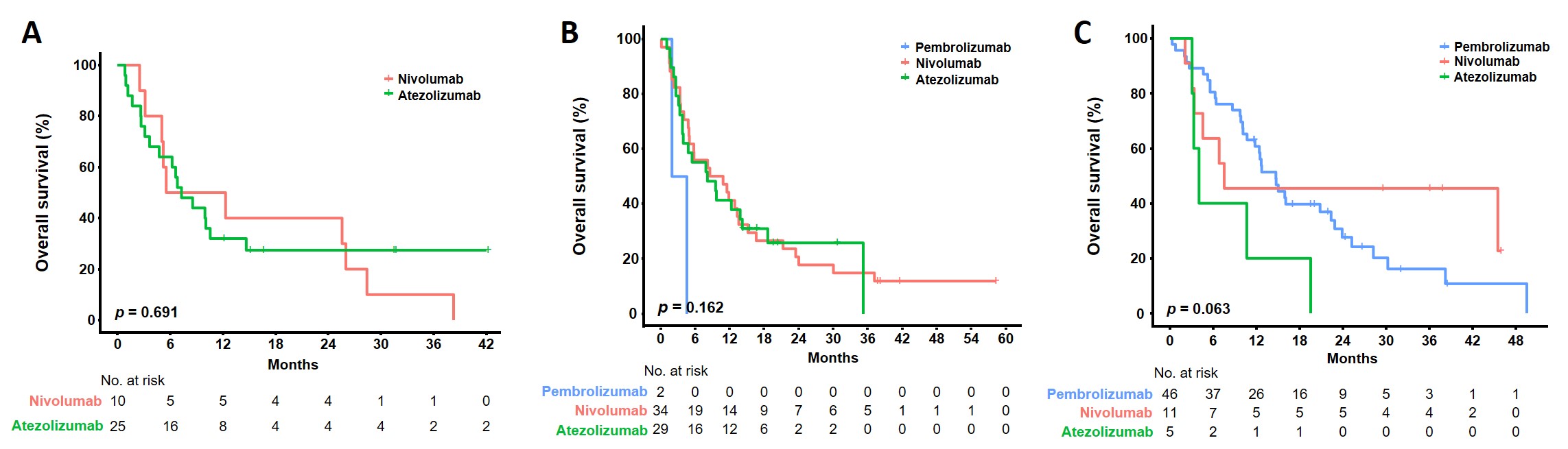
We classified a consecutive cohort of patients with advanced stage IV NSCLC into three groups according to the ICI monotherapy regimen. The three groups were older adults with an average age of ≥ 75 years, and some vulnerable patients with an ECOG-PS score of ≥ 2 were also included. For efficacy, the ORR were 22.4%, 8.2%, and 4.3% in the pembrolizumab, nivolumab, and atezolizumab groups, respectively, and pembrolizumab and nivolumab were more beneficial than atezolizumab. Nivolumab significantly improved ORR over atezolizumab when confirmed using correspondence analysis (nivolumab vs. atezolizumab, p = 0.006; pembrolizumab vs. atezolizumab, p = 0.471; pembrolizumab vs. nivolumab, p = 0.066). Similarly, DCR was better improved in the pembrolizumab (59.2%) and nivolumab (55.7%) groups than in the atezolizumab (30.0%) group. Similar results were observed in concordance analysis (nivolumab vs. atezolizumab, p = 0.003; pembrolizumab vs. atezolizumab, p = 0.005; pembrolizumab vs. nivolumab, p = 0.866). However, we cannot conclude that pembrolizumab and nivolumab are more effective than atezolizumab in terms of efficacy, and there are several reasons for this. First, patients who received atezolizumab showed more squamous histology than those who received other drugs did. As reported in several pivotal RCTs [6] and real-world outcome literature [23–25], squamous histology tends to be associated with shorter PFS and OS than non-squamous histology. Second, the present study did not treat each drug evenly according to PD-L1 expression. Following the existing pivotal RCT results, most patients with high PD-L1 expression were treated with pembrolizumab and nivolumab, and atezolizumab was mainly used in patients with low or unconfirmed PD-L1 expression in the present study. Therefore, patients in the atezolizumab group may show relatively poor efficacy. Despite these conditions, there were no differences in the OS among the three groups. The OS was 12.6 months, 8.4 months, and 7.7 months in the pembrolizumab, nivolumab, and atezolizumab groups, respectively, with pembrolizumab showing the longest trend. However, no significant differences were observed (p = 0.334). In addition, we confirmed the OS of patients receiving ICIs according to PD-L1 expression through correspondence analysis. In the PD-L1 expression group of 1–49%, when the OS according to ICIs was analyzed in correspondence, no statistical significance was observed (pembrolizumab vs. atezolizumab, p = 0.092; nivolumab vs. atezolizumab, p = 0.911; pembrolizumab vs. nivolumab, p = 0.053) (Supplementary Figure S1B). In contrast, in the PD-L1 expression group of ≥ 50%, pembrolizumab showed a statistically significant OS benefit over the atezolizumab (pembrolizumab vs. atezolizumab, p = 0.023; nivolumab vs. atezolizumab, p = 0.153, pembrolizumab vs. nivolumab, p = 0.406) (Supplementary Figure S1C). In the pembrolizumab group, eight patients treated as the first-line were included, and there were only five patients with PD-L1 expression of ≥ 50% in the atezolizumab group. Therefore, more samples are needed to determine statistical significance.
Older patients are likely to be vulnerable to the side effects of cytotoxic chemotherapy; therefore, they receive many ICIs that are known to have relatively tolerable side effects [26]. However, the eligibility criteria of clinical trials are not representative of the patient population in real-world practice, and most clinical trials use patients receiving conventional cytotoxic chemotherapy as controls. Therefore, data on the direct efficacy comparisons between ICIs are lacking.
A noteworthy finding of the present study was that bone metastases negatively affected OS. Bone is a hematopoietic organ based on cancer biology. It is involved in the production of regulatory T, memory T and B, and cytotoxic T cells that control the immune system [27, 28]. Therefore, pathological bone loss may impair immune-related cell production. The association between bone metastasis and survival has not been extensively studied; however, a prospective cohort study in Italy reported poor outcomes in terms of bone metastasis and survival rates [29]. In addition, several published retrospective studies have reported poor prognosis of bone metastasis [24, 30]. The present study’s results are consistent with those of previous studies indicating that bone metastases adversely affect the OS of patients receiving ICIs, and additional treatment methods or adjuvant agents that can enhance the efficacy of ICI in patients with bone metastasis need to be investigated.
This study had several limitations. First, as this was a retrospective single-center observational study, differences in the clinical baseline characteristics may have affected the efficacy evaluation. Pembrolizumab was used in the frontline and was administered more to patients with high PD-L1 expression. Therefore, these characteristics may have improved survival in the pembrolizumab group. Second, because various detection techniques are used to identify PD-L1 expression, the consistency between each method may be inaccurate. In the present study, three assays were used: PD-L1 22C3 pharmDx assay, VENTANA PD-L1 SP263, and VENTANA PD-L1 SP142 immunohistochemistry assay, and PD-L1 expression was classified based on the highest value among the three test results. Notably, not all three techniques were performed in all patients; therefore, unifying them into one technique was impossible. However, several studies have indicated that PD-L1 22C3 and SP263 techniques are highly consistent [31, 32]. In the present study, none of the patients had SP142 results reflected in the final result of PD-L1 expression. In addition, when only patients who underwent PD-L1 22C3 were analyzed for the accuracy of the results, there was no difference in OS according to ICI, as in previous studies (data not shown). Third, comorbidities were not considered in the survival study. In the case of older adults, comorbidities may affect survival; however, since the study was based on data from electronic medical records, information on comorbidities or the association between comorbidities and mortality could be overlooked. Despite these limitations, the survival outcomes in the present study were similar to those of the existing pivotal RCTs.
In conclusion, this study is clinically significant because no study has directly compared three different ICIs in older patients receiving ICI monotherapy. There were no statistically significant differences in survival outcomes among the three ICIs, demonstrating that they may be an appropriate treatment option for older patients. In addition, bone metastasis was associated with poor survival outcomes for immunotherapy.
{kind=link}