RET has become a frequently preferred treatment method in recent years, especially in necrotized immature teeth [18]. In the current literature, clinical studies evaluating the success of RET and studies examining the factors affecting the success of treatment (irrigation solutions, scaffolds used, appropriate indications) are the majority [19–21]. Coronary barrier materials are also one of the subjects studied by researchers. In the literature, there are studies evaluating the effect of material type on treatment success from various aspects (root length increase/apical diameter narrowing/increase in root thickness) [22]. However, the number of studies evaluating the biomechanical properties of RET-applied teeth is limited. In the literature, biomechanical properties have been evaluated mostly on the basis of fragility [23, 24]. Few studies have evaluated the biomechanical effect of materials on immature teeth by stress distribution [25, 26]. This is the first study in which the effects of using different thicknesses of MTA, CEM, and Biodentin for stress distribution in RET were evaluated together with FEA.
Simulation of traumatic forces in immature teeth is not ethically appropriate [12]. For this reason, in vitro studies comprise the majority of the literature. However, a complete simulation of the oral environment cannot be performed with in vitro studies [13]. Therefore, in the current study, stress assessment of traumatic forces was performed with FEA. In addition, a comprehensive examination was conducted by simulating all layers of the tooth and evaluating the stresses occurring in these structures separately. With FEA, a three-dimensional model was created by simulating the most realistic form of the tomographic image of the immature tooth. Thus, a more accurate assessment was provided. FEA studies give the same results each time they are repeated. Therefore, the obtained results were evaluated numerically and visually.
To study stress analysis with FEA, the modulus of elasticity and Poisson's ratio must be known. In Part 1, a contribution to the literature was made by calculating the values of the CEM with the nanoindentation test. The current study, using the values found in Part I, is the first FEA study to evaluate the stress caused by CEM applied in different thicknesses on dental tissues.
It has been reported in the literature that the application procedure of RET is not clear and that its deficiencies should be investigated [27]. Knowing the long-term results of studies on RET will enable clinicians to apply this treatment more safely [3]. This study will provide insight into how immature maxillary central tooth tissues and surrounding bone tissue are affected by secondary traumas after RET. In particular, immature teeth are fragile due to their underdeveloped root structures and weak cervical regions. [1]. Considering this situation, the effect of coronary barrier materials (MTA/Biodentin/CEM) applied in different thicknesses (3 mm/5 mm) in the cervical region on the stress distribution was evaluated in this study.
In a study in which the effect of MTA thickness on the stress distribution in RET was evaluated with FEA obtained lower stress values in the models in which RET was applied with a 5 mm thick material. This is in line with the results of the current study, compared to the control model [25]. In the current study, lower Von Mises stress values were obtained in dental tissues and bone tissue compared to the control model without RET, regardless of the thickness of the coronary barrier material (Tables 2 and 3). While Demirel et al. recommend the use of 5 mm material, in our study, there was no significant difference between the 3 mm and 5 mm groups. Therefore, we recommend using 3 mm of material in order to avoid excessive material use.
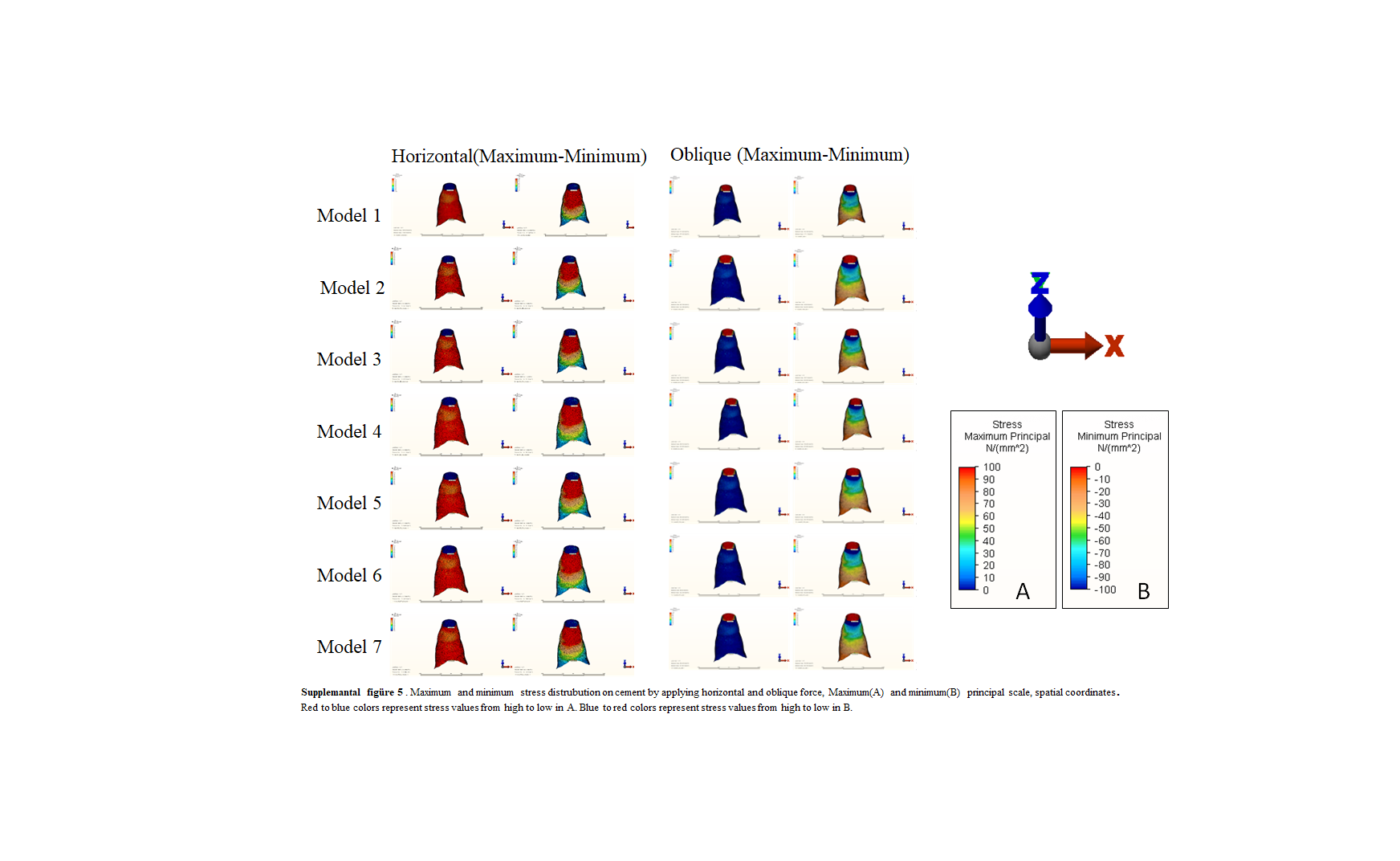
When the inner stress on the coronary barrier materials was evaluated, more stress occurred in the 5 mm models than in the 3 mm models. Considering the fragility of the materials, we can say that the use of 3 mm of material is more advantageous. When the materials were compared, the most inner stress occurred in CEM. The least inner stress occurred in the MTA. We can interpret these results as showing that CEM and Biodentin absorb more stress than does MTA.
Belli et al.[28] reported that restoration materials reduce the stress on dental tissues. Similarly the results of the present study revealed that the restoration materials applied in immature teeth reduce and distribute stress. Belli et al. obtained different results than the current study, finding that MTA transmits less stress than doesBiodentin. A similar result was obtained in an in vitro study evaluating the effects of CEM and MTA on fracture resistance. In our study, MTA transmitted higher stress to dental tissues. While CEM absorbed the most stress, Biodentin showed similar stress absorption to CEM. Complete standardization cannot be achieved with in vitro studies. This difference may be due to this [29].
Bucchi et al. simulated root dentin maturation after RET and compared the stress distribution in immature and mature teeth [2]. In the RET-applied tooth models, the researchers obtained lower stress values than in immature teeth. Similarly, in the results of the current study, lower stress values were obtained in dental tissues and surrounding bone tissue in all RET models compared to the control model. This situation can be interpreted as immature teeth becoming more biomechanically resistant with RET.
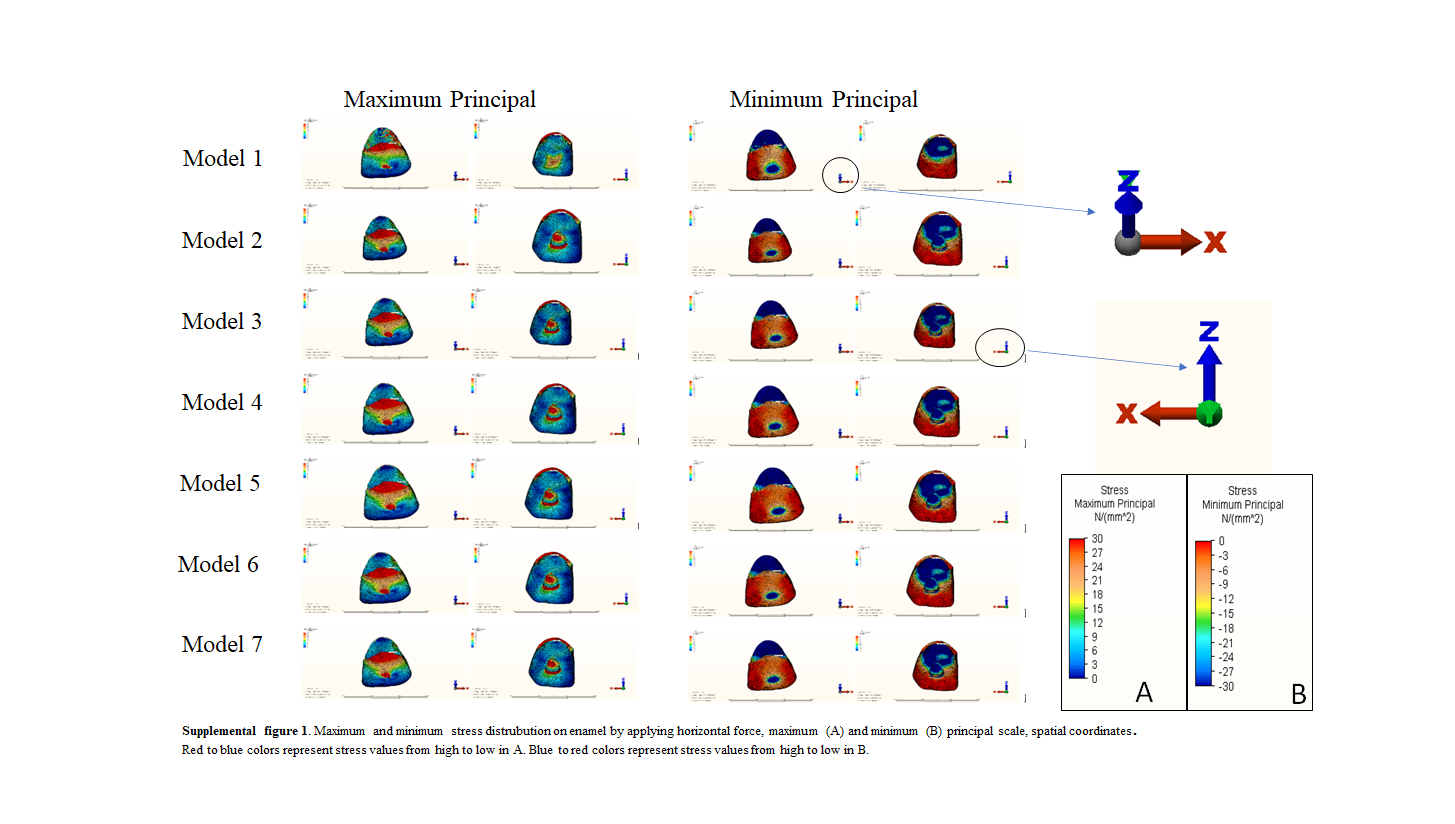
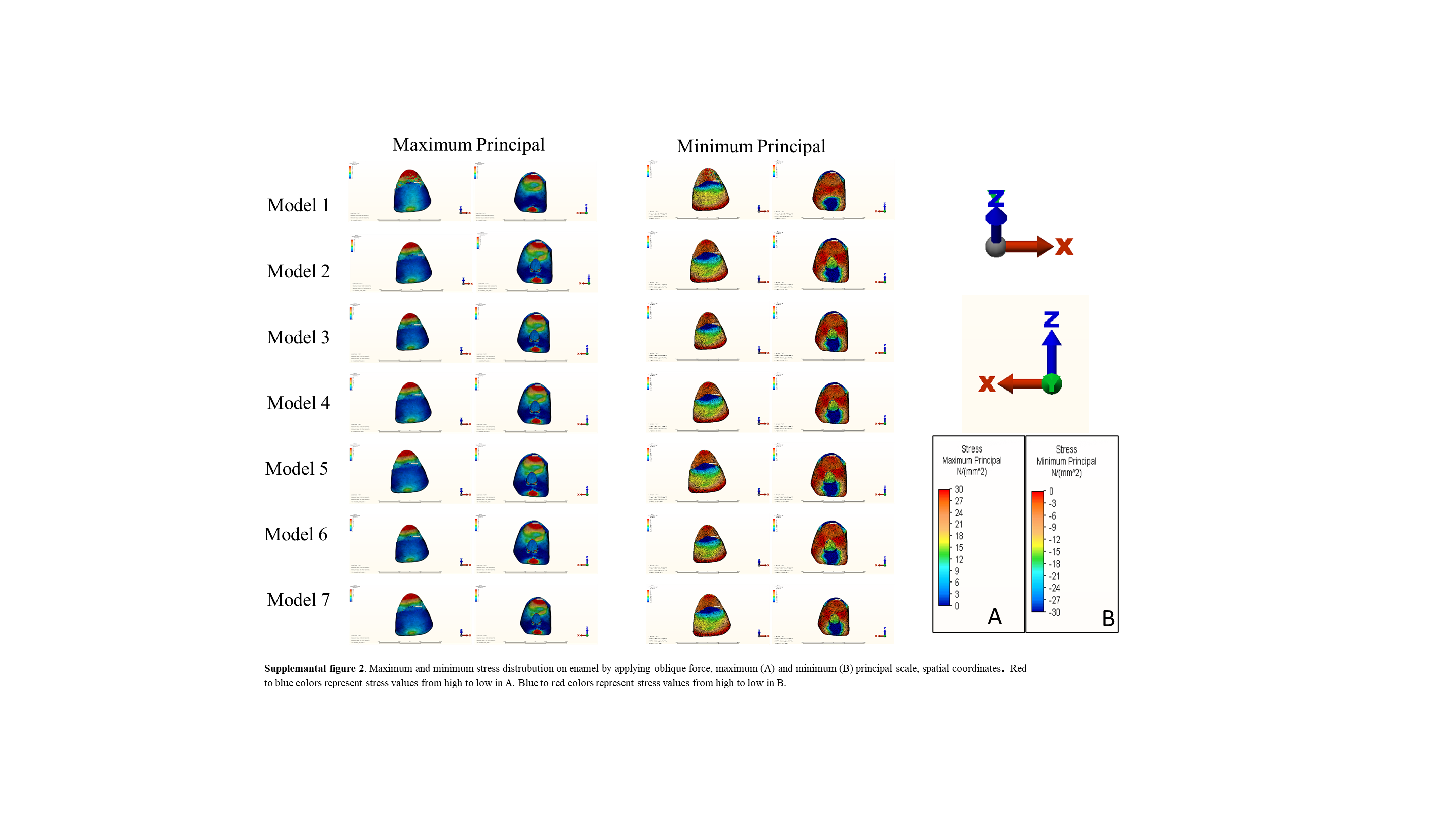
In the present study, as in the study of Poiate et al.[30], high tensile stresses occurred in the cervical region on the palatal surface of the enamel. The cervical region is also where the enamel is the thinnest, and this area should be supported in treatments for immature teeth [10]. Lower Von Mises stress values were observed in the enamel at the cervical region in all RET models compared to the control group. The lowest values were observed in the models (Models 5, 6, 7) in which 5 mm thick material was applied (Figs. 2, 3).
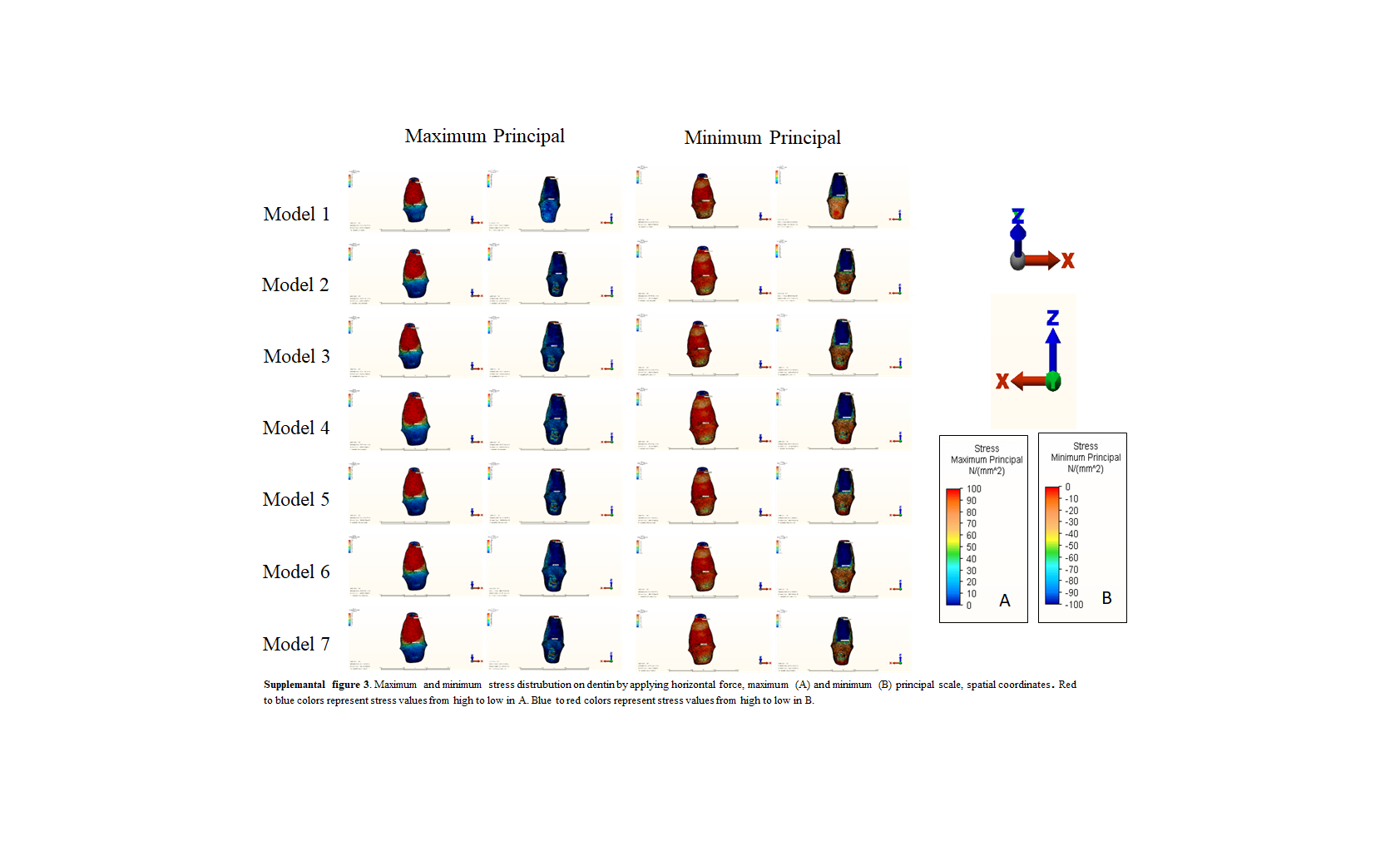
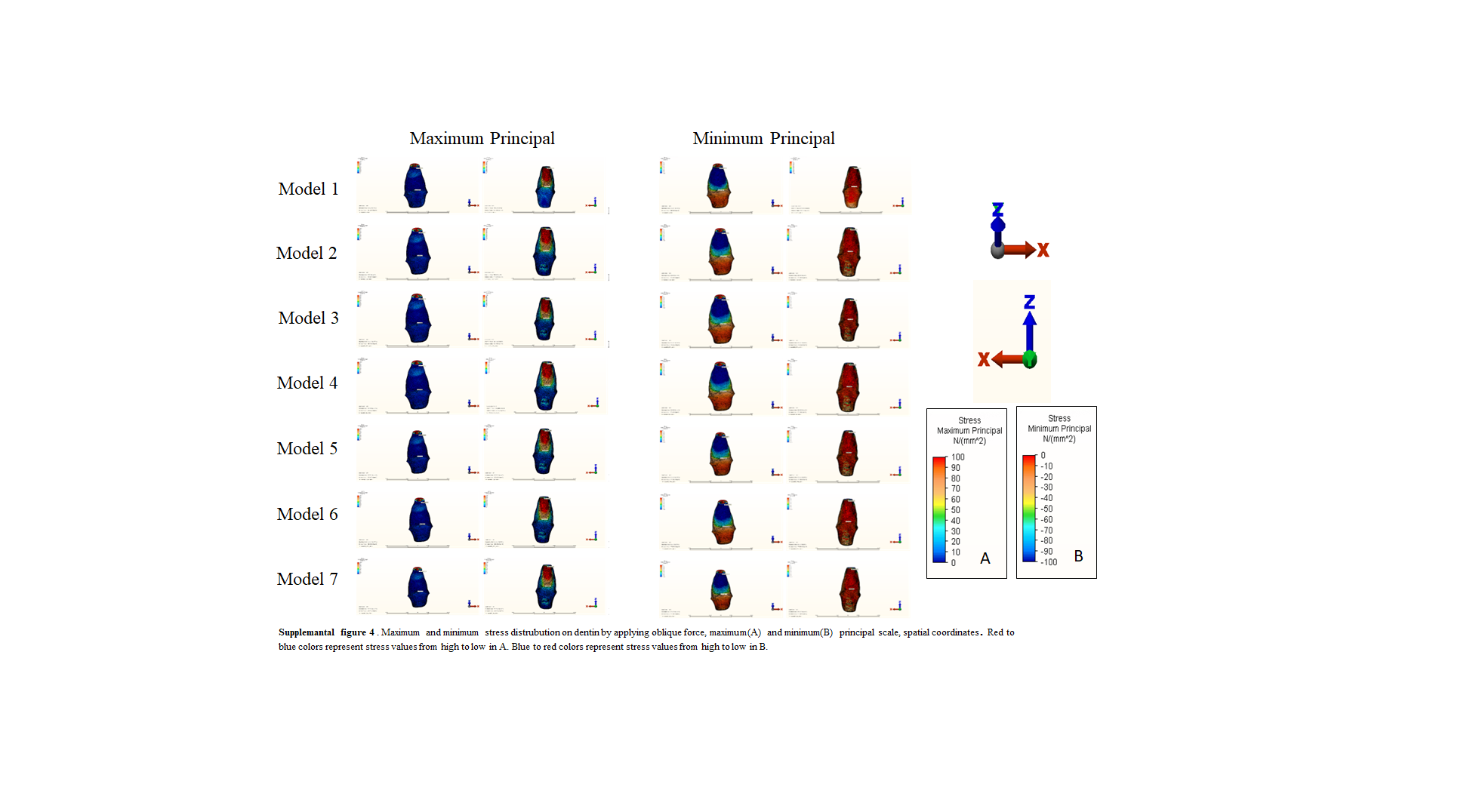
Maximum and minimum stress distribution were observed in the dentin in horizontal and oblique strength, increasing from the cervical region to the apex. This result indicates that stress is concentrated in the apex region of dentin in immature teeth, as in the study of Bucchi et al.Consistent with the results of the study conducted by Antrayoz et al. [31] in which they evaluated the stress caused by oblique force in the maxillary central tooth, the stress level in dentin decreased in all RET models compared to the control model. This result is similar to the results of our study. Stress analysis in models is promising for RET. Lower stress values were also obtained in cementum in the RET models compared to the control. Considering the fine structure of the cementum in immature teeth, the reduction in stress values is a valuable result for the long-term prognosis of immature teeth.
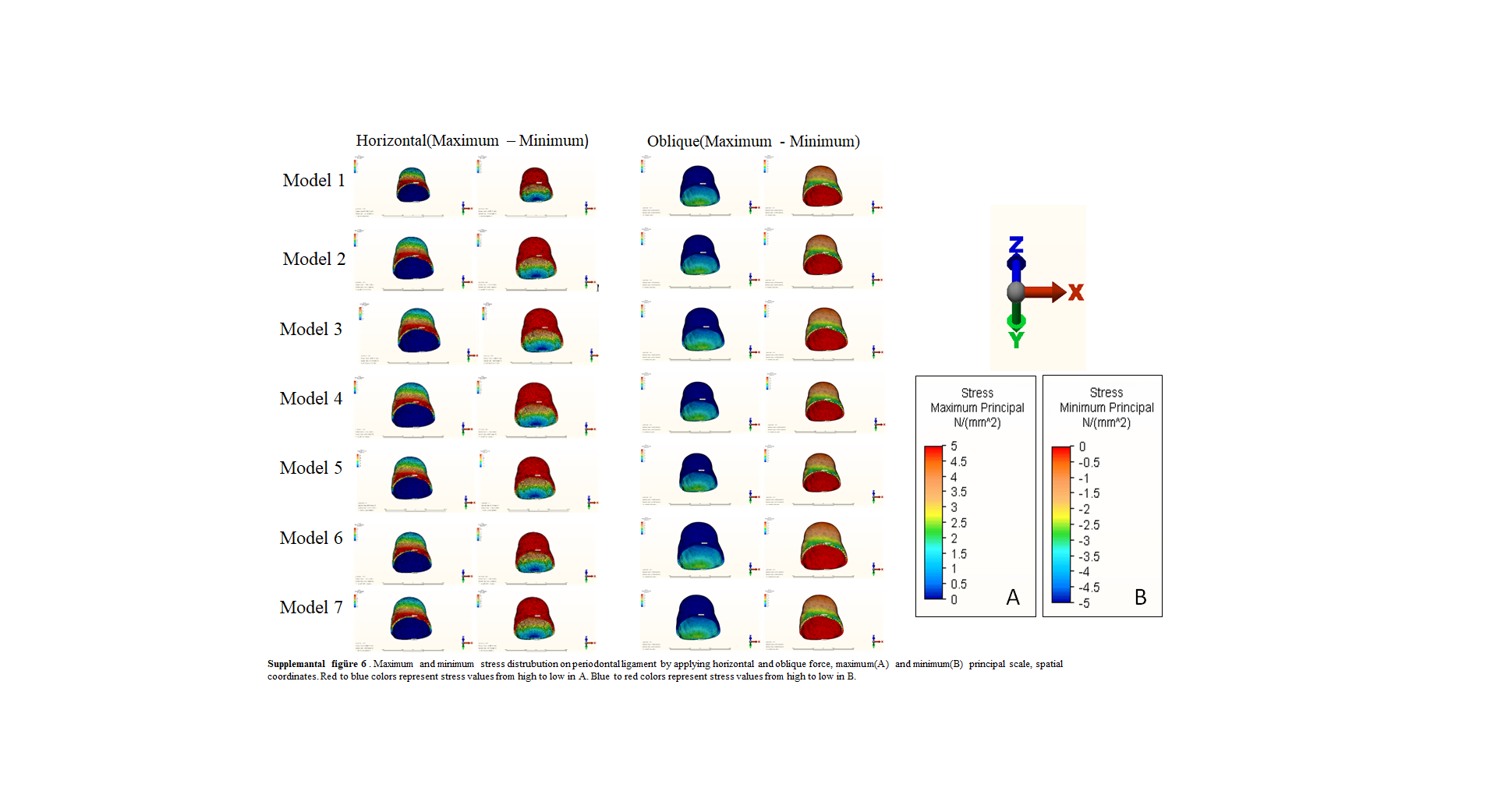
Tensile and compressive stresses are important for dental tissues and materials. The decrease in these values is an indication that the resistance of the teeth to the incoming traumatic forces has increased. In the current study, lower maximum and minimum principal values were obtained in the 5 mm models in enamel, dentin, cementum, and PDL.
Calcium hydroxide (CH) is used in the intermediate session in RET. CH is known to affect the modulus of elasticity of dentin. However, there are studies in the literature that say it reduces [32] fragility and studies that claim the opposite [33]. Since there are no definitive data on this situation, the change in modulus of elasticity in dentin after the use of CH was ignored in the study. In addition, the effects of the solutions used on the dentin tissue were ignored. These situations constitute the limitations of our study.
Calcium silicate-based cements are widely used in dentistry today. MTA is the most widely used. Various properties of these materials (setting time/compressive strength/surface microhardness/sealing ability/biological properties) have been investigated [34]. Biodentin and CEM are successful material that can be used in many areas where MTA is used. However, since there are not enough studies in these materials, they are less preferred than MTA [8]. In this study, the stress distribution in tooth and bone tissues, when applied in different thicknesses of MTA/Biodentin/CEM, was examined, and an idea about their biomechanical effects was provided. In models where CEM and Biodentin were used, the order of stress occurring in tooth and bone tissues was CEM < Biodentin < MTA. In an FEA study evaluating apexification using Biodentin, that material was found to be more successful in stress distribution in immature teeth than MTA [24]. In another study conducted with FEA on immature teeth, it was found that Biodentin, which is used at low thickness, is more advantageous than MTA [23].
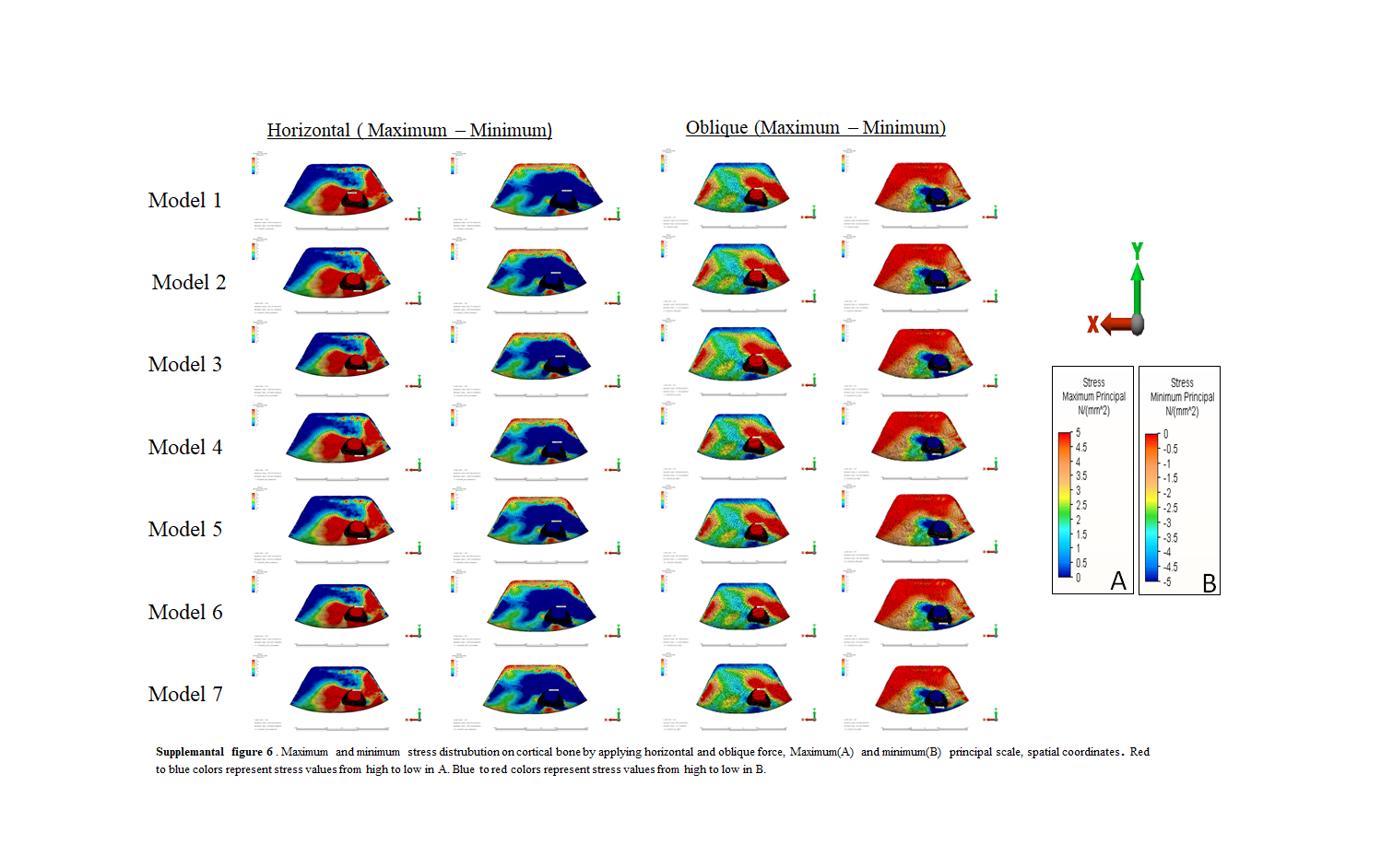
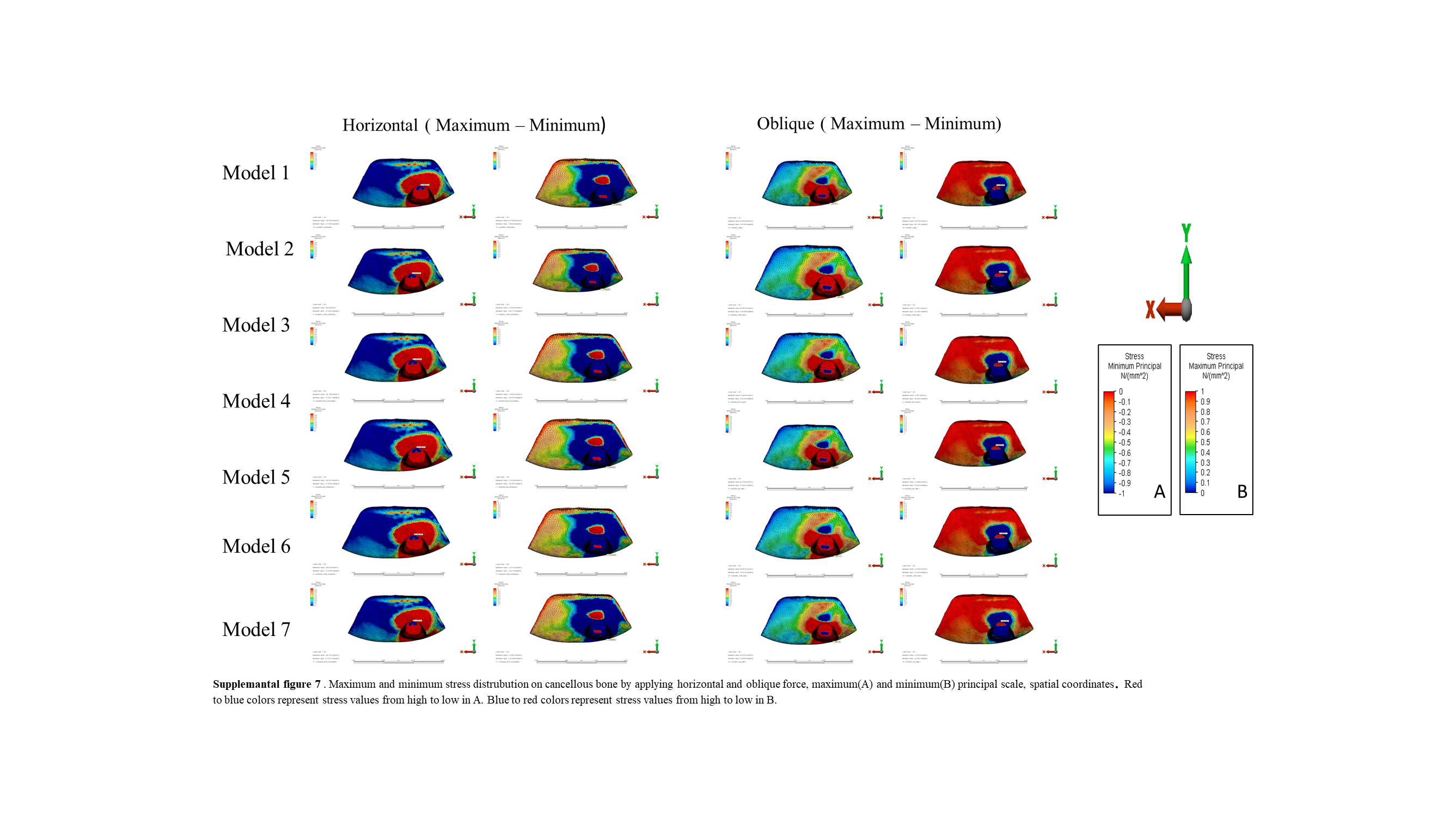
Although the stress distribution in cortical and cancellous bone was similar, fewer maximum and minimum principal values were obtained in the RET models. The stress values obtained on the 5 mm models were less than on the 3mmmodels. However, there was no significant difference between them. In PDL, lower stress values were obtained in the RET models than in the control model. This is an indication of reduced stress in bone tissue. The lowest stress values were obtained in CEM models, as in other dental tissues. This result constitutes important proof of the usability of CEM.
The effect of restorative materials on treatment success is important [2]. In the current study, a full RET simulation was performed by including restorative materials (glass ionomer/composite) and all tooth/bone tissues in addition to coronal barrier materials. This situation constitutes the difference between our study and others in the literature.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}