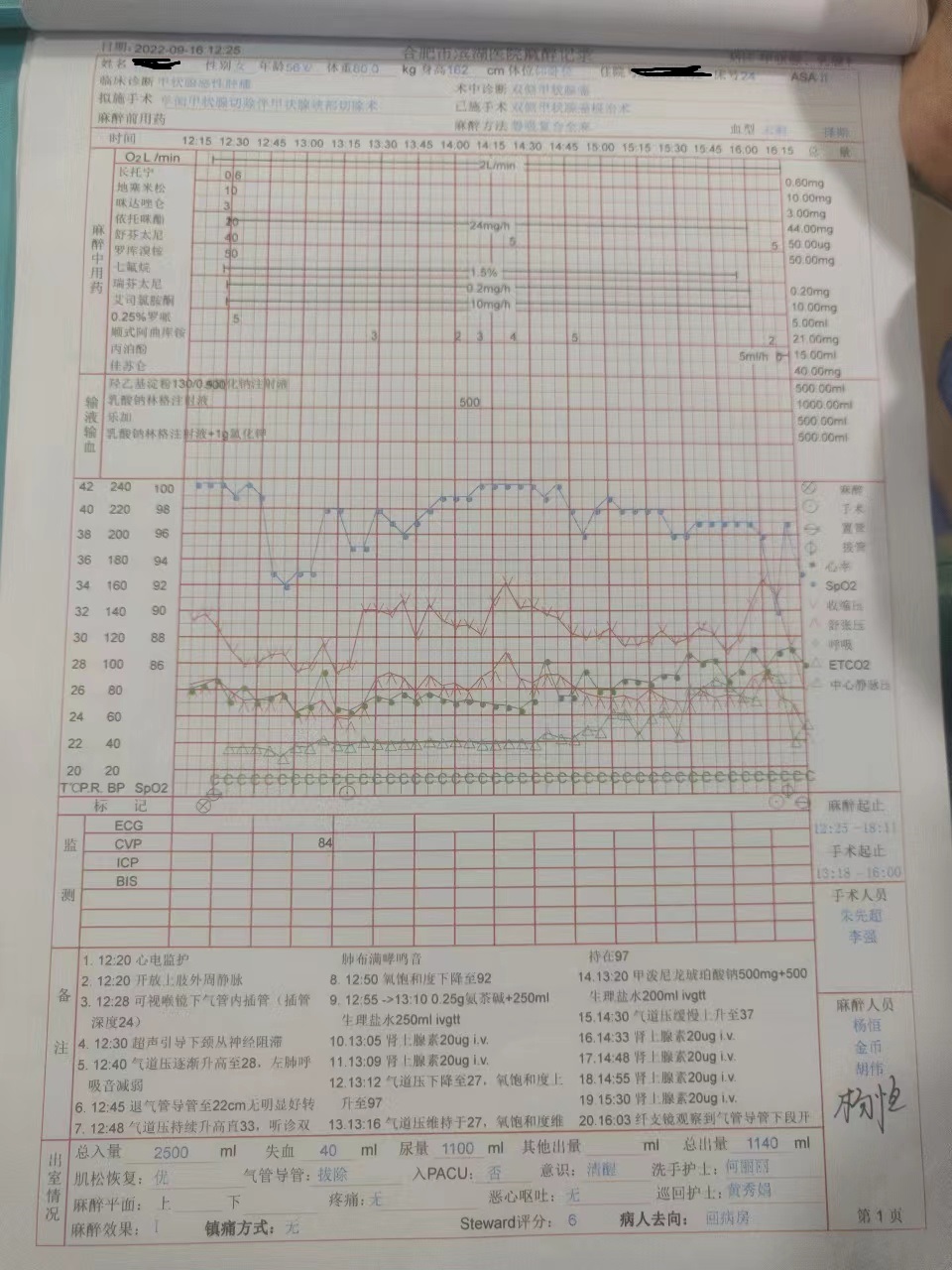
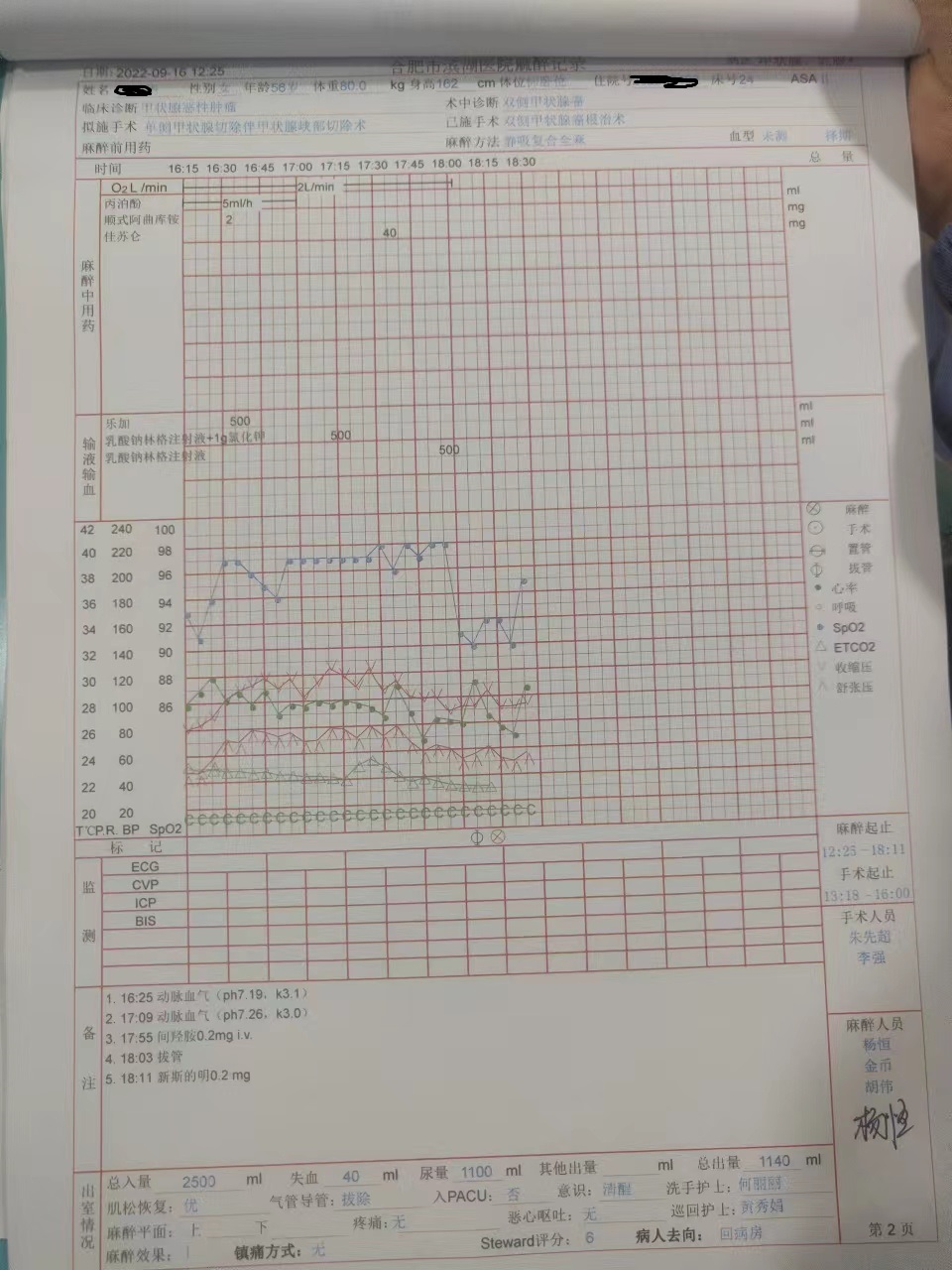
The patient was a 56-year-old female with 162 cm height, 80 kg weight, and 30.5 kg.m-2 body mass index (BMI). Because of thyroid nodules, she underwent bilateral radical thyroidectomy under general anesthesia in our hospital. Her mouth opening was three fingers with Mallampati grade II and no apparent complex airway manifestations. Her chief complaint was a prolonged history of chronic pharyngitis. There was no history of asthma, smoking, or recent upper respiratory tract infection. Preoperative lung CT showed fibrous lesions and calcifications in the upper lobe of the left lung. Except this, respiratory and circulatory systems were normal, and liver and kidney function tests were within normal ranges. She had ASA grade II according to the American Society of Anesthesiologists (ASA) standard.Anesthesia and treatment:After fasting for eight hours, routine monitoring was performed in the operating room. Non-invasive blood pressure was 132/84 mmHg, heart rate was 80 beats.min-1, and pulse oxygen saturation was 99%. After regular rehydration and oxygenation, anesthesia was inducted using penehyclidine hydrochloride 0.6 mg, dexamethasone 10 mg, midazolam 3 mg, sufentanil 40 µg, etomidate 20 mg, and rocuronium 50 mg. After anesthesia induction, tracheal intubation was successfully performed using a video laryngoscope. The tip of the tracheal tube was 23 cm away from the incisor. The ventilator was set to volume ventilation mode, tidal volume was set to 450 mL.time-1, and frequency was set to 14 times.min-1, airway pressure was 18 cmH2O, and oxygen saturation was 100%. After maintaining anesthesia for about five minutes, the airway pressure gradually increased to 28 cmH2O, and the breathing sound of the left lung decreased in auscultation. Subsequently, we withdrew the endotracheal tube to 22 cm, and auscultation was repeated. At this time, wheezing was heard in all foci of auscultation, airway pressure rose to 33 cmH2O, and oxygen saturation decreased from 100–92%. Considering the occurrence of bronchospasm, the oxygen flow was immediately increased, and 0.25 g aminophylline was given intravenously. In addition, 500 mg methylprednisolone sodium succinate was given intravenously. The symptoms did not significantly improve after five minutes, and 20 µg epinephrine was given intravenously. After two consecutive injections, airway pressure decreased to 27 cmH2O, oxygen saturation reached 97%, and patient's condition became stable. After consulting with family members, it was decided to continue the operation. Approximately one hour after the initiation of the surgery, airway pressure gradually increased to 37 cmH2O. Epinephrine 20 µg was injected intravenously, and repeated several times as the response was not satisfactory. Her airway pressure remained at 37 cmH2O and did not significantly decrease during manual ventilation. Oxygen saturation was held at 93%, and we requested the surgeon complete the surgery as soon as possible. At the end of the process, the lungs were auscultated immediately, and it was found that the respiratory sounds were weakened, and no obvious wheezing sound was heard. The endotracheal tube was immediately examined and found that it was not significantly compressed or broken. Finally, we used fiber bronchoscopy and found that the lower end of the endotracheal tube was blocked by a yellow object, and we could not remove it with the suction tube. The new endotracheal tube was immediately replaced, and moderate positive end-expiratory pressure (PEEP) was performed. The PEEP value was set to eight cmH2O. At the same time, arterial blood was extracted for blood gas analysis. After tracheal tube replacement, the patient's airway pressure immediately decreased to 16 cmH2O, and her oxygen saturation increased to 98%. The results of arterial blood gas analysis were as follows: PH: 7.19, PaCO2: 65 mmHg, PaO2:83 mmHg, K+: 3.0 mmol L-1, and Lac: 2.3 mmol L-1. We immediately replenished liquid and potassium chloride, increased minute ventilation volume, and simultaneously performed intermittent lung expansion. After 30 minutes, blood gas analysis showed that PH: 7.26, PaCO2: 51 mmHg, PaO2: 106 mmHg, K+: 3.1 mmol L-1, and Lac: 3.6 mmol L-1. We continued symptomatic and supportive treatment. After the operation, the patients were observed for about one hour. The patients' self-consciousness and respiratory function rapidly recovered, and the sputum was successfully removed. About one hour after the surgery, the patient had no apparent complications or discomfort and was safely sent back to the ward. The yellow object in patient's tracheal tube was a long strip and covered about 70% of the tube area. After the operation, it was sent to the pathology department for examination. The pathological results reported that it contained mucus and scattered mild columnar epithelium, tissue cells, and a few neutrophils. One night after the surgery, the patient had mild sore throat and vomiting twice, and there were no other complaints. After a week of follow-up, the patient recovered without complications and was then discharged.
{kind=link}
{kind=link}