Impact of triple therapy on attenuating the luminal dilatation of AAA (Fig. 1)
The baseline of abdominal aortic diameter at infra-renal level did not differ among the six groups. However, by day 14 after AAA induction, the AAA diameter was lowest in group 1 (SC), highest in group 2 (AAA only) that was identically reduced in groups 3 (AAA + DAPA), 4 (AAA + entresto), 5 (AAA + ADMSCs) and 6 (AAA + DAPA + entresto + ADMSCs). Additionally, by day 28 after AAA induction, this parameter was lowest in group 1, highest in group 2, significantly lower in group 6 than in groups 3 to 5, and significantly higher in group 5 than in groups 3 and 4, but it showed no difference in the latter two groups. Our finding implicated that any one therapy was better than AAA without treatment and triple therapy was superior to merely one on reduction of AAA diameter.
Impact of triple therapy on attenuating the intimal hyperplasia of AAA by day 28 after AAA induction (Fig. 2)
To elucidate whether triple therapy could effectively suppress the intimal hyperplasia of AAA, the light microscopic finding of H.E. stain was done. The result showed that intimal hyperplasia was lowest in group 1, highest in group 2, significantly reduced in group 6 than in groups 3 to 5 and significantly reduced in group 5 than in groups 3 and 4, but it showed no difference between the groups 3 and 4.
Impact of triple therapy on attenuating the fibrosis of AAA by day 28 after AAA induction (Fig. 3)
To verify whether the triple therapy could significantly attenuate the fibrosis in AAA, Masson’s trichrome staining for identifying the fibrotic cross-section area of AAA was utilized in the present study. The result showed that the percentage of fibrotic cross-section area was lowest in group 1, highest in group 2, significantly higher in group 3 than in groups 4 to 6, and significantly higher in groups 4 and 5 than in group 6, but it was similar between groups 4 and 5.
Impact of triple therapy on protecting the small vessel density in abdominal aortic cross-section layer by day 28 after AAA induction (Fig. 4)
To determine whether the number of small vessels increased in AAA, we utilized the α-SMA staining. The result demonstrated that the number of small vessels (defined as diameter ≤ 25 µm) was highest in group 1, lowest in group 2, significantly lower in group 3 than in groups 4 to 6, and significantly lower in groups 4 and 5 than in that of group 6, but it showed no difference between groups 4 and 5.
Impact of triple therapy on protecting the integrity of smooth muscle layer in abdominal aortic cross-section layer by day 28 after AAA induction (Fig. 5)
To clarify whether the triple therapy would effectively protect the integrity of smooth muscles in medial layer of abdominal aorta, SM22-α staining was conducted in the present study. The result showed that the damaged score of smooth muscles in medial layer of AAA was significantly lowest in group 1, highest in group 2, significantly lower in group 6 than in groups 3 to 5 and significantly lower in groups 4 and 5 than in group 3, but it was similar between groups 4 and 5.
Impact of triple therapy on suppression of cellular expressions of immune cells in AAA by day 28 after AAA induction (Fig. 6)
To clarify whether triple therapy would inhibit the cellular expressions of immune cells, the microscopic examination of IHC stain was utilized in the present study. The result demonstrated that the cellular expressions of CD3 + and CD4 + cells, two indices of immune cells, were lowest in group 1, highest in group 2, significantly lower in group 6 than in groups 3 to 5, and notably lower in group 5 than in groups 3 and 4, but they were similar in groups 3 and 4.
Impact of triple therapy on suppression of cellular expressions of inflammatory cells in AAA by day 28 after AAA induction (Fig. 7)
To verify the cellular expression of inflammation, IHC staining was utilized in the present study. The result showed that the cellular expression of MMP-2, an indicator of inflammation, was lowest in group 1, highest in group 2 and significantly lower in group 6 than in groups 3 to 5, but it showed no difference among the latter three groups.
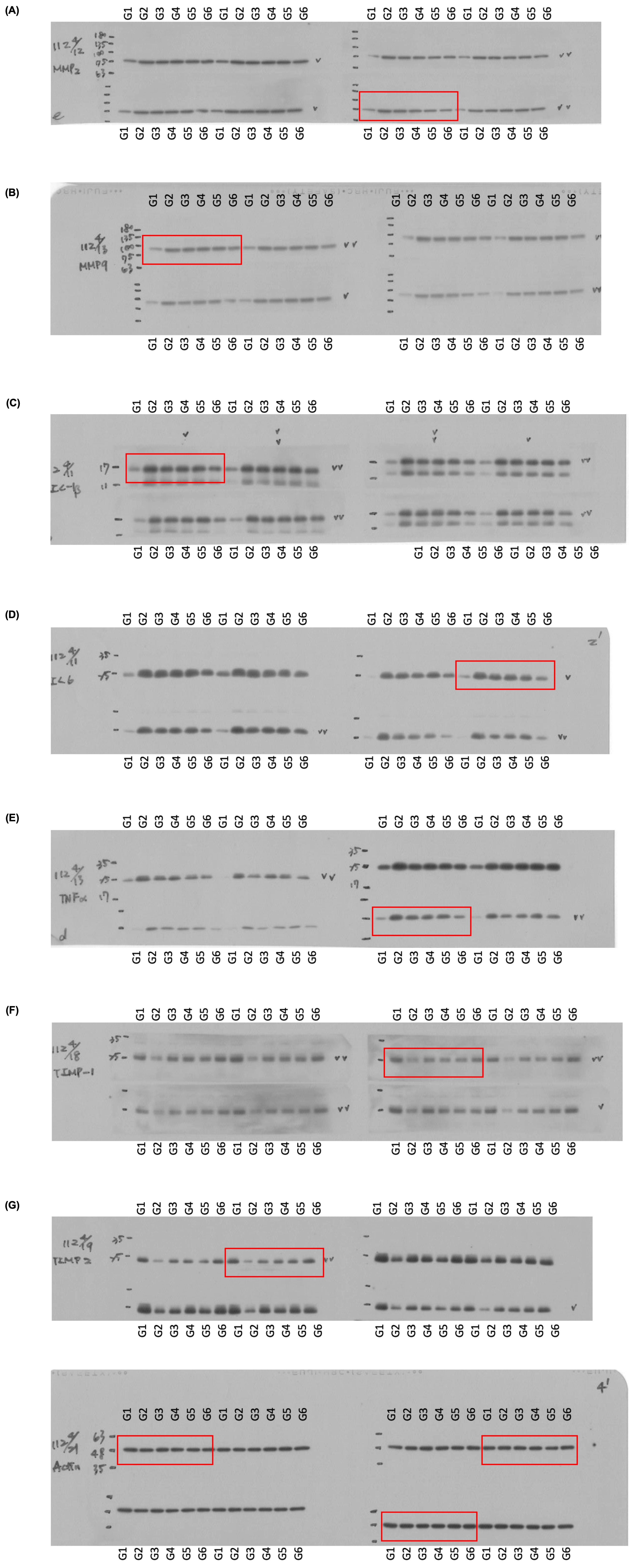
Protein expressions of inflammation in AAA by day 28 after AAA induction (Fig. 8)
To verify whether triple therapy could effectively suppress the inflammatory reaction, the Western blot analysis was conducted in the present study. The result showed that the protein expressions of MMP2, MMP9, IL-1β, IL-6 and TNF-α, five indicators of inflammation, were lowest in group 1, highest in group 2, and significantly lower in group 6 than in groups 3 to 5, but they were similar among the latter three groups, whereas the protein expressions of TIMP1 and TIMP2, two matrix metallopeptidases, displayed an opposite manner of inflammation among the groups. Our findings implied that triple therapy was better than just one therapy on attenuating the protein level of inflammatory reaction.
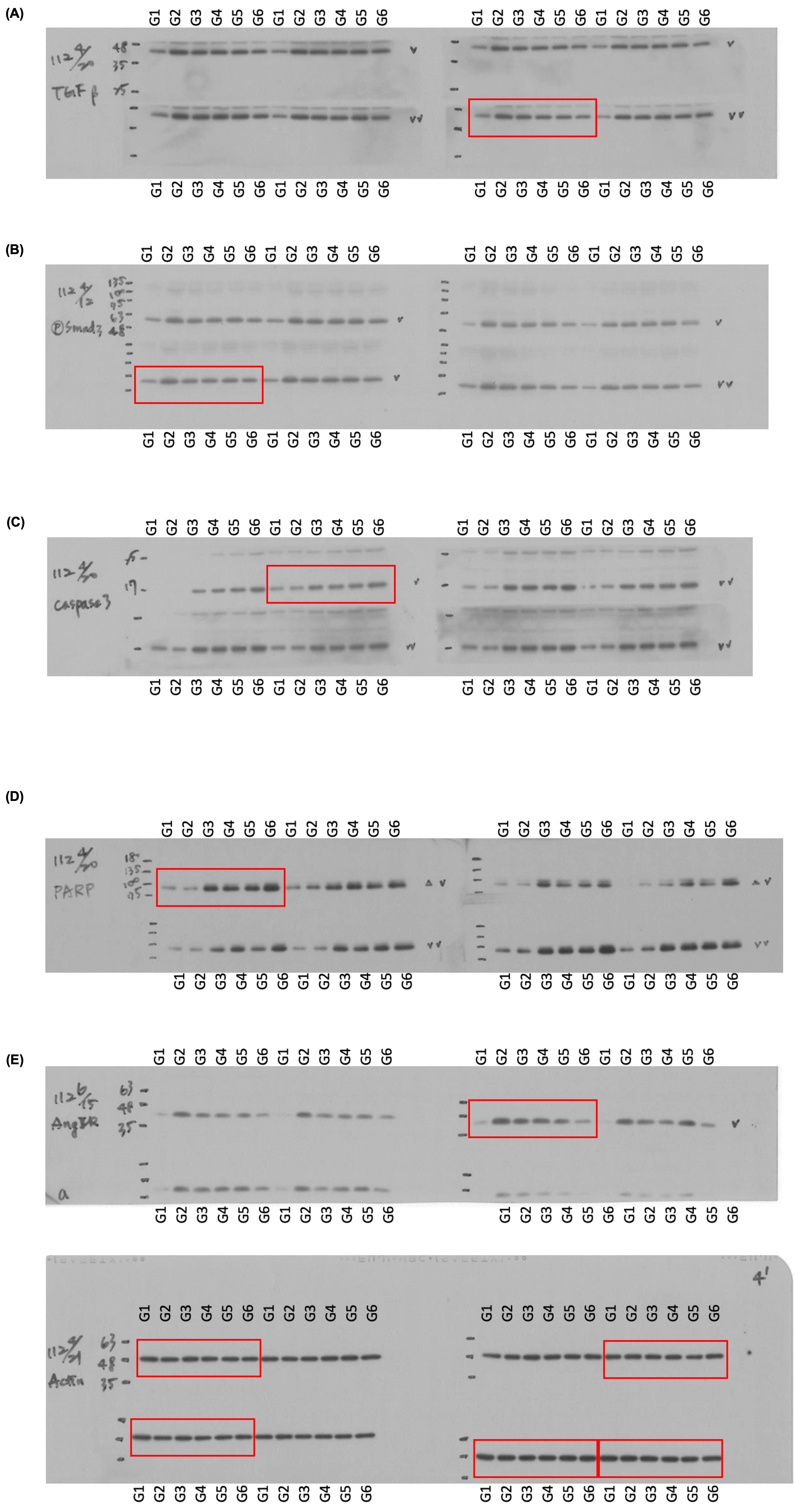
Protein expressions of apoptotic, fibrotic and angiotensin II receptor biomarkers in AAA by day 28 after AAA induction (Fig. 9)
Once again, we utilized the Western blot for determining the protein levels of apoptosis, fibrosis, and angiotensin II receptor. The results demonstrated that the protein expressions of TGF-β and p-Smad3, two indices of fibrosis, protein expressions of cleaved Caspas3 and cleaved PARP, two indicators of apoptosis, and protein expression of angiotensin II receptor, an indicator of RAAS activation, were lowest in group 1, highest in group 2, and significantly lower in group 6 than in groups 3 to 5, but they were similar among the latter three groups.
{kind=link}
{kind=link}