Study Participants
Young healthy male adults with type 1 diabetes with no microvascular complications or cardiovascular risk factors were recruited from diabetes out-patient clinics in Lothian, Scotland. Men without diabetes, matched for age, were recruited by poster advertisements and from a database of volunteers. Only male subjects were studied to avoid the confounding effect of the variability of coronary flow reserve that occurs during the menstrual cycle (21). In addition, because the counterregulatory hormonal responses to hypoglycemia differ between men and women (22), the study was confined to men to avoid a potential effect of gender on the magnitude of the sympatho-adrenal stimulus during hypoglycemia.
Exclusion criteria included co-existent systemic disease, malignancy, chronic alcoholism, psychiatric disorder, any history of cardiac conduction abnormality, impaired awareness of hypoglycemia (as assessed by the method of Gold et al (23)), past history of severe hypoglycemia, and any evidence of overt microvascular complications including retinopathy and neuropathy or the presence of microalbuminuria.
A total of 17 male adults with type 1 diabetes and 10 age-matched individuals without diabetes were studied (Table 1). Participants with type 1 diabetes had reasonable glycemic control, (average glycated haemoglobin (HbA1c): 8.0±1.1%; 64+11 mmol/mol), with a median duration of diabetes of 15 years (range 2-35 years), which is consistent with average quality of glycemic control recorded in the adult population with type 1 diabetes in Scotland. The two groups of participants did not differ in age or body-mass index (Table 1).
The study was conducted with informed written consent of all subjects, the approval of the Lothian Medical Research Ethics committee, and in accordance with the Declaration of Helsinki.
Study Design
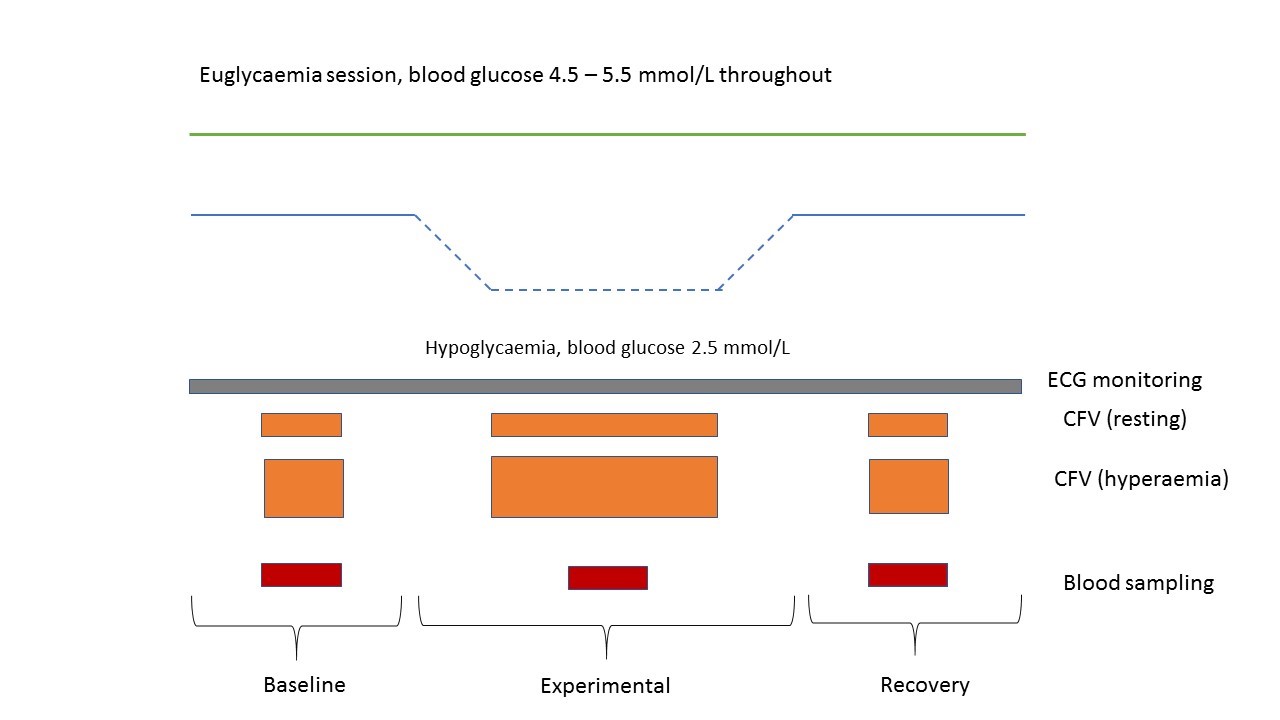
Participants attended for two study visits, performed on separate days at least two weeks apart to avoid any potential carry-over effects. Two experimental conditions, hypoglycemia (blood glucose 2.5 mmol/L; 45 mg/dL) and euglycemia (4.5 mmol/L; 81 mg/dL), were studied in a prospective, randomised, open-label, blinded endpoint, (PROBE) cross-over study. Both the group with type 1 diabetes and matched individuals underwent the experimental conditions, and then crossed-over. The order of the experimental method was randomized using alternate randomization by the operator of the glucose clamp, while the endpoint was blinded to the echocardiographer (Supplemental figure 1). This study design has been employed previously by our group (24), with modifications for the cardiovascular investigations.
Participants attended in a fasting state, having abstained from consumption of caffeine-containing food and beverages for 24 hours. Venous cannulae were inserted for intravenous infusion of dextrose and insulin, and blood sampling. A modified version of the hyperinsulinemic glucose clamp was employed (25). To arterialize blood samples, the non-dominant arm was wrapped in a heated blanket with a retrograde intravenous cannula inserted into the forearm. An additional cannula was inserted into the non-dominant antecubital fossa to infuse insulin (human Actrapid; Novo Nordisk, Crawley, U.K.) and 20% dextrose. Insulin was infused at a constant rate of 1.5 mU/kg/min with a Gemini PCI pump (Alaris Medical Systems, San Diego, CA). Blood samples were taken at 5-min intervals and analyzed by a glucose oxidase method (2300 STAT; YSI, Yellow Springs, OH). The dextrose infusion rate was adjusted to maintain the appropriate arterialized blood glucose concentration. During a run-in period, arterialized blood glucose was maintained at 4.5 mmol/L (81 mg/dL) for 20 min. Blood glucose was then either maintained at 4.5 mmol/L (81 mg/dL) throughout (the euglycemia condition), or lowered over 20 min to 2.5 mmol/L (45 mg/dL) (the hypoglycemia condition), and maintained at this level for 30 min before restoration of euglycaemia. During the glucose clamp, the participants underwent an ultrasound examination by a trained ultrasound operator, using a well-described technique (16,21). The timepoints were labelled as baseline, experimental (either euglycemia or hypoglycemia-blinded to the sonographer), and recovery (Supplemental Figure 1). Continuous electrocardiographic monitoring and regular blood pressure monitoring were performed throughout the study.
Coronary Flow Velocity Measurements
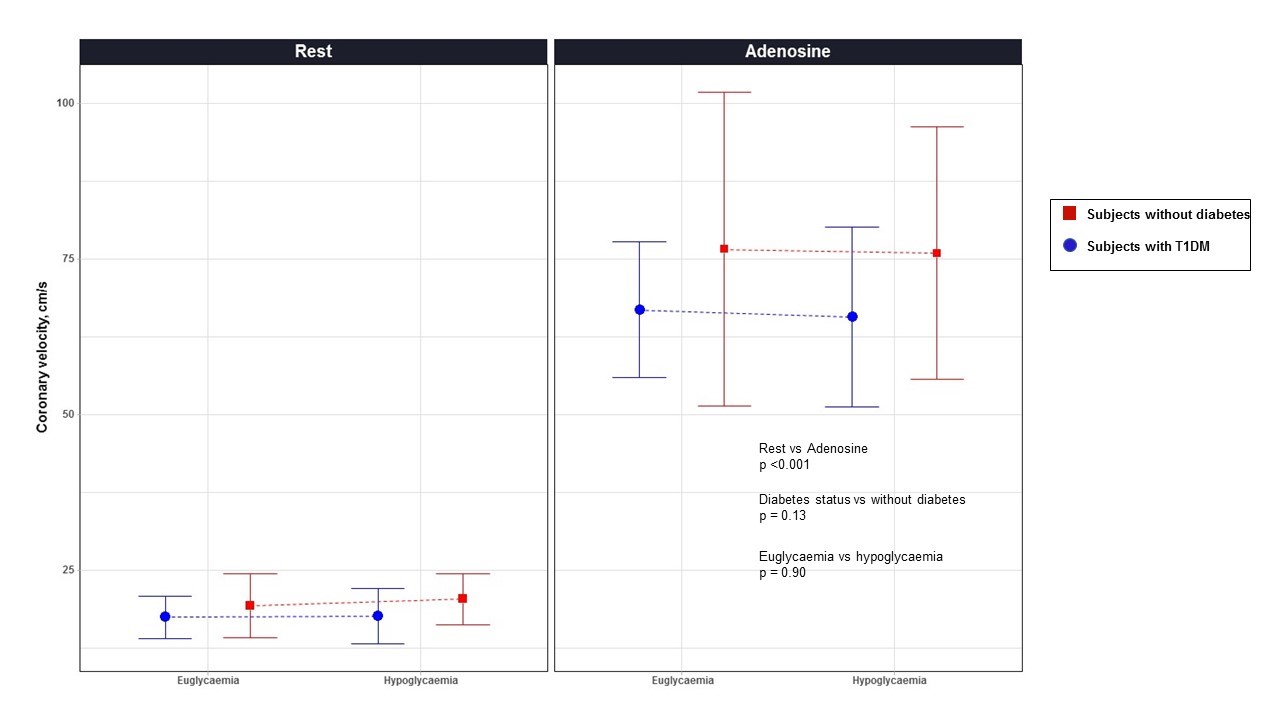
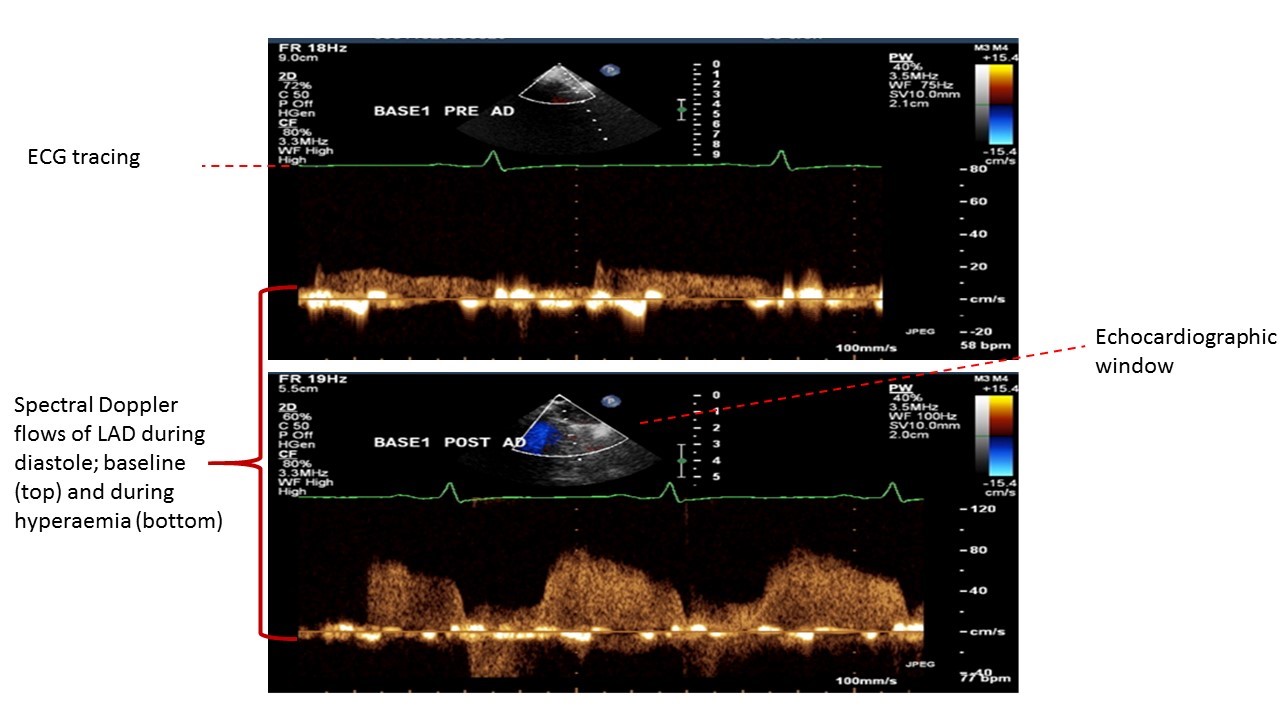
During each study condition, the left anterior descending coronary artery was visualized by trans-thoracic echocardiography. Transthoracic Doppler echocardiography was used for a non-invasive estimation of coronary flow velocity (CFV), and maximal coronary vasodilatation was induced with an adenosine infusion to allow calculation of CFR. Imaging of the left anterior descending (LAD) artery and measurement of coronary blood flow velocity was performed using a 7.0 MHz transducer (Acuson Sequoia 512, Siemens Medical Solutions, Berkshire, UK). Baseline spectral Doppler signals were recorded initially in the distal portion of the LAD coronary artery over five cardiac cycles at end-expiration. To measure coronary flow reserve (CFR), intravenous adenosine was administered (0.14 mg/kg/min; Adenocor, Sanofi) for up to 4 min to record spectral Doppler signals during hyperemic conditions (14). Coronary velocities were measured at baseline and at peak hyperemic conditions from the Doppler signal recordings. Measurements were averaged over three cardiac cycles. CFR was defined as the ratio of hyperemic to basal velocities, using maximum velocity (Vmax) parameters (Supplemental Figure 2). Blood pressure was recorded at baseline, during adenosine infusion and at recovery. CFR was calculated at baseline, during the experimental phase (0-20 min) and in the recovery phase.
High-sensitivity Cardiac Troponin I Concentration
Blood samples were taken prior to assessment of CFR, during the experimental hyperinsulinemic clamp, and during the recovery period (Supplemental Figure 1). High-sensitivity cardiac troponin I concentrations were determined using the ARCHITECT STAT high-sensitive troponin I assay (Abbott Laboratories, Abbott Park, IL). This is the first clinically approved high-sensitivity troponin I assay, which has excellent precision at very low concentrations. The limit of detection is 1.2 ng/L and precision profiling in our laboratory has demonstrated an inter-assay coefficient of variation (CV) of <10% at 5 ng/L. The upper reference limit or 99th centile is 16 ng/L for women and 34 ng/L for men (26-28).
Statistical Methods
A power calculation was performed using results from a previous study using a similar technique (29), a sample size of 12 allows an 80% chance of detecting a 0.57 difference in CFR, which is considered clinically relevant. The effects of hypoglycemia on coronary flow reserve were assessed statistically by generalized linear mixed-effects modeling, with the experimental condition (hypoglycemia and euglycemia) and diabetes status as variables affecting CFR. Statistical significance was taken as a two-sided p<0.05. Unless specifically stated, results are mean + standard deviation. The hsTnI data were log-transformed due to the skewed distribution. Heart rate, blood pressure, glucose and troponin data were analyzed using paired t-tests. Analysis of the results was performed using R stats (Version 3 for Windows and MacOS, R Foundation, USA).
{kind=link}
{kind=link}
{kind=link}