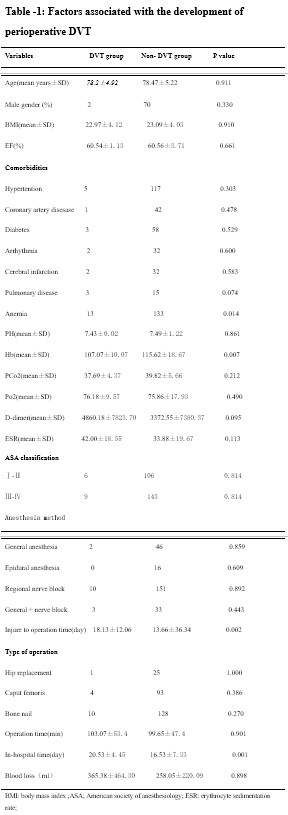
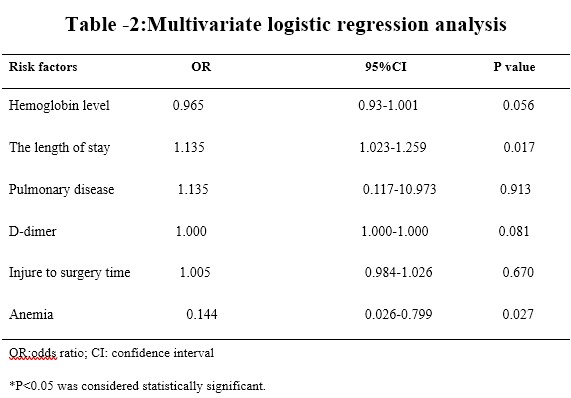
This study demonstrated that the overall incidence of DVT after hip fracture was 5.6%, and no PE occurred in all patients. In addition, multivariate logistic regression analyses indicated that pre-operative anemia and hospitalization time were the independent risk factors for preoperative DVT after hip fracture. However, 3.4% of patients underwent the surgery within the 48 hours after the fracture.
Hip fracture is one of the most common orthopedic conditions. The risk of VTE in patients with hip fracture is massive, which is the second most frequent complication of surgery. Previous research has shown that, in the absence of VTE prophylaxis, total and proximal DVT rates were approximately 50% and 27%, respectively [2]. Reboerts et al[3] and Hefley et al[4] have reported that the incidence of DVT was about 6%–9% in patients with hip fracture. They have pointed out that the main risk for these results was delayed surgery. In addition, Wong et al have been reported that the incidence of VTE was 6.4% after proximal hip fracture in Singapore[5]. Mok et al have also reported that the incidence of VTE was 8% after proximal hip fracture in Hong Kong[6]. All above results are the same to our results. What’s more, there was an epidemiological study about the DVT rate after major orthopedic surgery in Asia, which has indicated that the rate of DVT observed after hip fracture surgery(42%) was similar to those reported in western patients(36–60%), but the rate of proximal DVT was lower (7.2% vs 17–36%)[13]. After reviewing all these papers, it seems prudent to perform surgery as early as possible in order to improve the recovery and reduce peri-operationthe mortality, morbidity and other complications, preferably within the 48 hours after the fracture.
Unfortunately, in this study, only 3.4% of patients were undergoing surgery within the 48 hours after the fracture. Delayed surgery for these kinds of patients is known to be one of the most important factors contributing to the high incidence of preoperative DVT [4]. The guidelines from the United States and Canada have recommend that hip fracture surgery should within the 48 hours after the fracture [14]. The same study has also pointed out that waiting time longer than 24 hours was associated with the higher risk-adjusted likelihood of 30-day mortality(6.5% vs 5.8%)[15]. However, multi-disciplinary consultation and preoperative evaluation are often required owing to the prevalence of severe comorbidities in these patients. They are often delayed for 48 hours or even have preoperative DVT. In clinical work, targeting within the 48 hours, even in the 24 hours, represents a significant change in practice because 66% of the patients did not receive surgery within time frame [15]. But it is difficult to according this standard, especially in the developing country. In a prospective epidemiological study in the 19 centers across Asia, the time between hip fracture and surgery mean days was 11.0±12.4 in patients undergoing elective orthopedic surgery[13].
Globally, the prevalence of anemia is 12.7% for men and 23.9% for the elderly [16], which is associated with worse outcome [17]. However, the incidence of anemia at admission in individuals with hip fracture is high, varying from 12.3% with hemoglobin level less than 10 g/dL to 40.4% with hemoglobin level less than 12 g/dL[18]. Even over half the patients with hip fracture are anemic at admission [19]. Anemia in patients with hip fracture is closely related to increased mortality, prolong admission, higher readmission rate and increased mortality rate [20]. Halm et al. have observed the anemia (hemoglobin<12.0 g.dl) at admission in 40.4% of 550 patients with hip fracture, and reported that anemia at admission was related to hospitalization time and death or readmission with the 60 days [21]. The lower hemoglobin level at admission is not owing to bleeding from trochanteric fracture, but reflects the anemia before the injury. Anemia contributes to and is connected with reduced physiological reserve, function and mobility [22], which may increase VTE risk and prolong hospitalization time. Smith et al have reported that the average delay of surgery was 5.7 days for patients with DVT versus 3.2 days for those without DVT (p = 0.021)[22]. Recently study has also indicated that preoperative anemia (Hemoglobin<10.0 g/dl) was independently associated with lower 6-mouth functional scores and lower physical health-related quality of life scores for hip fracture surgery[24]. Preoperative anemia in individuals undergoing orthopedic surgery is associated with perioperative blood transfusion, which can be connected with longer hospital stays[25]. Furthermore, most patients in this study often had cardiovascular disease before surgery, which reminded that we should actively correct perioperative low hemoglobin to reduce the risk of cardiovascular events.
Hip fracture is common, costly, and often associated with poor outcome among older adults. It is logical to perform surgery as early as possible in order to avoid these complications. However, a longer period of preoperative evaluation and optimization will always be necessary. Besides, more and more evidence have suggested that comprehensive geriatric assessment decreased the risks of complications after hip fracture[26]. Reducing hospitalization time including early discharge to home or rehabilitation facilities can reduce the high case-fatality rate and healthcare costs, and increase the numbers of available public hospital beds[27]. The aim of lowering the costs of hospital-based care must be balanced against the clinical needs of the patients. Nordstrom et al have also pointed out that the shorter hospitalization time after hip fracture was associated with increased risk of death after discharge[28]. At present, in most areas of China, elderly with hip fracture are mainly treated with home rehabilitation after discharge, which leads to the lack of professional medical guidance in the early postoperative period. European and North American studies have shown that care provision by more nurses with at least bachelor’s degrees are associated with lower mortality after surgery[29–30]. A previous study has also pointed out that the mean postoperative length of stay was 5 days in the USA and 34 days in the Japan, and the risk of death after hospital discharge was doubled in the USA in comparison with Japan[28]. Therefore, in practice, the costs and benefits need to be assessed on a case-by-case basis, not just the emphasis on the bed conversion and medical costs. Furthermore, it is necessary to change the concept that hip fracture has been described as geriatric disease rather than orthopedic disease. Comanaged geriatric fracture center program that has resulted in lower than the predicted hospitalization time and readmission rates, with short time to surgery, low complication rates and low mortality [31–32]. Kammerlander et al. have been pointed out that the interdisciplinary team could achieve the lowest in-hospital mortality rate(1.14%), the lowest hospitalization time (7.39 days) and the lowest mean time to surgery(1.43 days)[33].
limitations
This study was a single-center retrospective analysis and all data were retrospectively collected. A multi-center randomized controlled trial is needed in the future.
{kind=link}
{kind=link}