We evaluated the prognostic utility of early-on levels of hs-cTnT, copeptin and NT-proBNP for all-cause mortality at 30-days follow-up in clinically characterized patients with OHCA of assumed cardiac origin, presenting with asystole or VF.
NT-proBNP was found to be significantly related to death in univariate analysis, whereas hs-cTnT and copeptin were not associated with outcome. Adjusting for demographic- and clinical variables, the prognostic value of NT-proBNP was attenuated and no longer statistically significant.
These findings are consistent with two previous studies [24, 25], reporting a similar association between admission levels of NT-proBNP and outcome in resuscitated OHCA patients. There are several possible mechanisms for increased NT-proBNP/BNP secretion during cardiac arrest and CPR, including hypoxemia [30], ischemia [31], ischemia-reperfusion induced inflammation [32], therapeutic interventions with administration of fluids [33] and vasopressors [34], and mechanical ventilation with supplementary oxygen administration [35]. Myhre et al. 2016 [24] demonstrated an increase in NT-proBNP levels from admission up to 96 hours after hospitalization in OHCA-VT/VF patients. Longer time to ROSC and higher admission levels of hs-cTnT were found to be associated with high NT-proBNP concentrations after 24 hours in multivariable analysis. Furthermore, 24-hour NT-proBNP levels provided additional prognostic information for the prediction of 1-year mortality. These associations may reflect myocardial changes brought about by the cardiac arrest, whereas earlier on-site levels of NT-proBNP in our study most likely will reflect the pre-cardiac arrest condition, as patients in Q4 as compared to lower quartiles were more prone to heart failure, were older and presented with worse renal function. Accordingly, NT-proBNP levels did not differ between on-scene non-ROSC patients and those who died in hospital. The prognostic value of comorbidity has previously been claimed to be of less importance in OHCA patients [36, 37], and this may explain the lack of prognostic utility for early-on NT-proBNP in our study. However, early measurements of NT-proBNP may help to identify OHCA-patients with clinically silent heart insufficiency or coronary artery disease, in need of special medical attention.
Demographic- and clinical factors, such as age, witnessed cardiac arrest, bystander-initiated CPR, primary heart rhythm and time to ROSC, are previously found to be prognostically important in cardiac arrest [3, 38-42]. Furthermore, plasma concentrations of NT-proBNP are known to be associated with age and kidney function [13]. Multivariable analysis, adjusting for these established risk-variables, cancelled the significant univariate association between early-on levels of NT-proBNP and outcome. However, in accordance with previous observations [3, 39 – 42], we also noted that increasing age and longer duration of CPR was significantly associated with increased risk of death, while witnessed cardiac arrest and VF as primary heart rhythm was associated with a more favourable outcome (Figure 3).
In contrast to previous reports [3, 39], bystander-initiated CPR was not found to be an independent outcome-predictor in our study, probably cancelled by a larger proportion of VF-patients and a short EMS response-time between 8 to 15 minutes in our recruitment area.
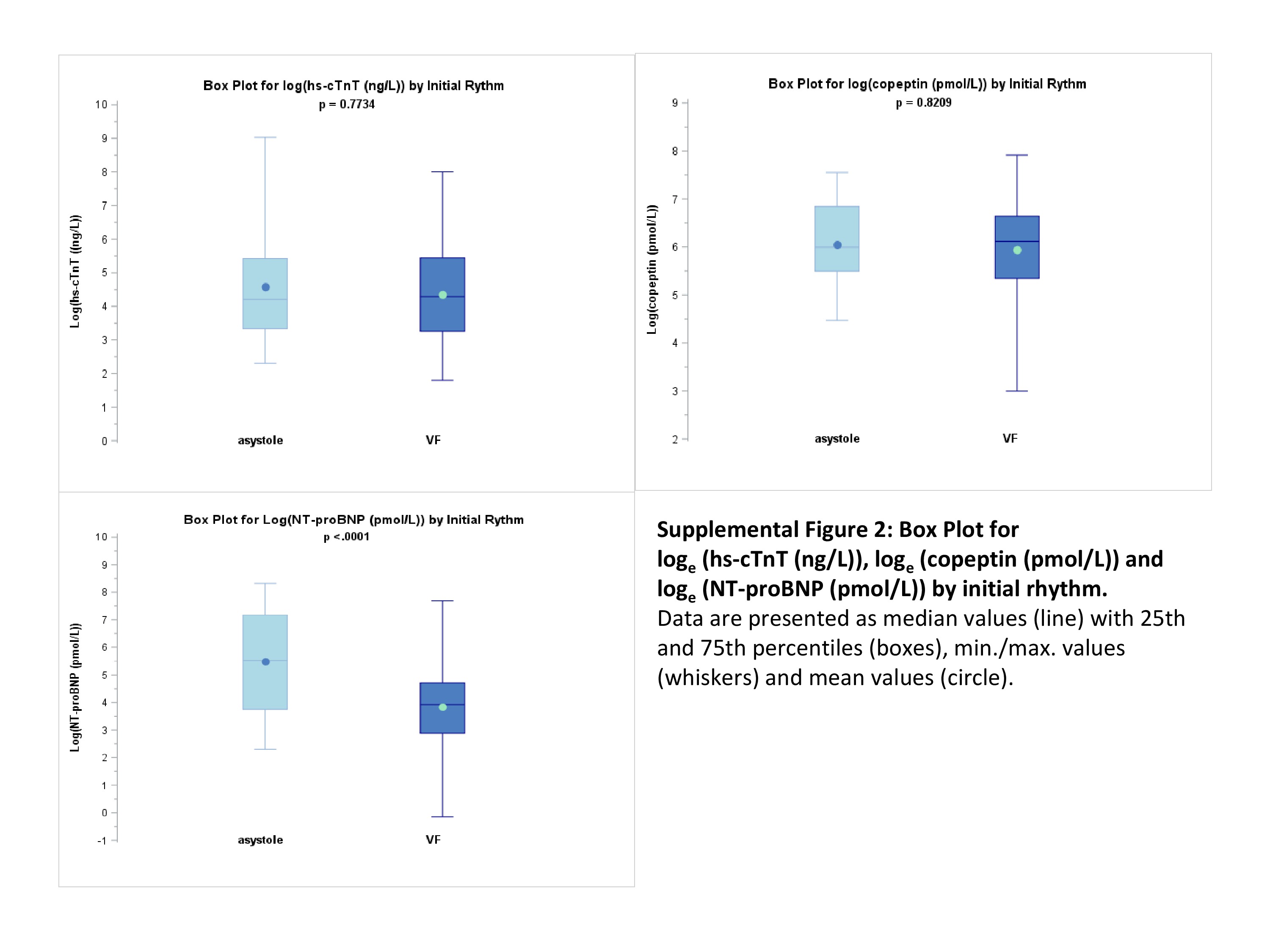
Furthermore, we found that NT-proBNP differentiated between ischemic VF patients and those presenting with asystole. This could be explained by a difference in baseline risk variables, as previously reported [21]. Patients in the asystole group were older and a higher proportion suffered from prior cardiac morbidity, including established coronary artery disease and heart failure. However, no difference in NT-proBNP was observed when comparing non-ischemic VF patients with those presenting with asystole. These groups had similar baseline characteristics and differed mainly by the presenting arrhythmia, which may relate to prognosis. Accordingly, all patients in the asystole group died as compared to 50% in the non-ischemic VF group.
The two other biomarkers, hs-cTnT and copeptin, were not related to outcome, neither in univariate, nor in multivariable analysis. As previously demonstrated [9], we found that essentially all resuscitated OHCA-patients had elevated levels of hs-cTnT. Gilje et al. [20] found that hs-cTnT peaked 24 hours after admission following OHCA, but only hs-cTnT at 48 and 72 hours, respectively, was independently associated with all-cause mortality. In our study, we analysed only one blood sample very close to the cardiac arrest, which may not reflect the peak values of hs-cTnT, and the prognostic utility may have been missed. This assumption is supported by the FINNRESUSCI substudy by Røsjø et.al [9], where admission levels of hs-cTnT failed to differ between hospital non-survivors and survivors and did not yield independent prognostic information at 1-year follow up in OHCA-VF/VT patients.
Copeptin levels were markedly increased in all patients in our study and did not differ between 30-days non-survivors and survivors. Admission levels of copeptin have previously been demonstrated to independently predict organ dysfunction and death in the ICU following OHCA [22]. As a predictor of long-term mortality, copeptin levels at day 3 were shown to perform better than copeptin measured at ICU-admission [23]. In our early-on sample, elevated copeptin may largely reflect the stress response during cardiac arrest, rather than outcome related hemodynamic instability following ROSC. The prognostic utility of copeptin claimed in the FINNRESUSCI population [22], is based on samples harvested up to 6 hours after admission and did not include on-scene non-ROSC patients.
Strengths
Blood was collected very early after OHCA and includes non-admitted patients without ROSC, a patient category usually missed out in previous studies. Also, the initial cardiac rhythm was recorded in all patients. Pre-hospital data were collected in accordance with the Utstein guidelines [26], and advanced cardiac life support was performed by the EMS paramedics according to current guidelines [27].
Limitations
The small study population is one of the limitations. Further studies with larger patient populations should be performed to assess the prognostic value of these three biomarkers. Inclusion of patients was restricted to the largest ambulance centres in the area located closest to the hospital and to the medical support helicopter to ensure timely delivery of blood samples, limiting the potential recruitment area. Furthermore, patient recruitment could only be performed when there was enough EMS crew present at the OHCA-scene. Samples were obtained during resuscitation and not after death was declared. Unfortunately, there was a selection bias due to unbalanced blood sampling in the ROSC and non-ROSC group of patients. A few patients lacked detailed information regarding the OHCA. Our study is limited to 30-days observations of outcome.
{kind=link}