A total of 603 participants aged 5 to 88 (median: 32; interquartile range (IQR): 42) years were examined in 12 clusters (communities) of the six Health Areas of the Ndikinimeki Health District. The sex ratio (M/F) was 1.04 (proportion of males: 50.9%).
Prevalence and intensity of O. volvulus infection
Of the 603 participants examined, 42 (7.0%; 95% CI: 5.2–9.3%) were found to be infected with O. volvulus. The prevalence of onchocerciasis was significantly higher in the Boutourou Health Area (21.6% (95% CI: 14.5–30.1%) (χ2 = 48.708, df = 5, P = 0.0001), among males (11.1%; 95% CI: 7.7–15.1%) (χ2 = 16.301, df = 1, P = 0.0001) and among younger adults (20–34 years-old) (18.3%; 95% CI: 11.0–27.6%) (χ2 = 25.727, df = 3, P = 0.0001) (Table 1). At the community or cluster level, onchocerciasis prevalence ranged between 0% (95% CI: 0–8.8%) and 23.7% (95% CI: 13.6–36.6%). A significantly higher burden of the disease was observed in the communities Kiboum 1 (19.3%; 95% CI: 10.0–31.9%) and Kiboum 2 (23.7%; 95% CI: 13.6–36.6%) compared to the other communities (highest prevalence in Makénéné Town Water: 8.5%; 95% CI: 2.3–20.4%) (P = 0.0001) (Fig. 1) (Table 2) (Additional file 1: Table S1). Furthermore, a significantly higher prevalence of the disease was observed among farmers (P = 0.0001).
The overall microfilarial density was 0.557 ± 3.784 (mean ± SD) mf/ss, significantly higher in the Boutourou Health Area (χ2 = 47.576, df = 5, P = 0.0001), among males (Mann Whitney U-test: U = 41645.5, Z = -4.016, P = 0.0001) and young adults aged 20–34 years (χ2 = 25.703, df = 3, P = 0.0001) (Table 2). The intensity of infection was also significantly higher in Kiboum 1 (1.395 ± 8.414) and Kiboum 2 (1.814 ± 5.199) communities compared to other communities (highest microfilarial density in Makénéné Town Water: 0.979 ± 4.264) (χ2 = 50.490, df = 11, P = 0.0001). The overall CMFL in the study area was 0.168 mf/ss, significantly higher in the Kiboum 1 (0.383 mf/ss) and Kiboum 2 (0.538 mf/ss) communities (Additional file 1: Table S1).
Morbidity associated with onchocerciasis
The overall prevalence of palpable nodules was 0.3% (95% CI: 0.1–1.2%), ranging between 0–0.6% but the difference was not significant between Health Areas (χ2 = 1.416, df = 5, P = 0.923), communities (χ2 = 8.768, df = 11, P = 0.643), age groups (χ2 = 2.892, df = 3, P = 0.409) and gender groups (χ2 = 0.001, df = 1, P = 1).
The overall prevalence of skin depigmentation and rashes was 3.0% and 0.3%, respectively, and no significant difference (P > 0.330) was found between Health Areas (χ2 = 5.762, df = 5, P = 0.330). The difference was also not significant between gender groups (χ2 = 0.154, df = 1, P = 0.694), age groups (χ2 = 1.037, df = 3, P = 0.792) and clusters (χ2 = 9.015, df = 11, P = 0.620).
Regarding pruritus, the proportion of individuals affected was significantly higher in the Nyokon Health Area (26.9%; 95% CI: 16.8–40.3%) compared to the other Health Areas (χ2 = 21.925, df = 5, P = 0.001), the difference was also significant when considering clusters (χ2 = 92.731, df = 11, P < 0.0001) and age groups (χ2 = 18.498, df = 3, P < 0.0001), but the difference was not significant when considering gender (χ2 = 1.436, df = 1, P = 0.231).
History and adherence to ivermectin treatment
Overall, 74.8% (95% CI: 71.2–78.1%) of participants reported that they have swallowed ivermectin at least once during the past 5 years. The proportion of individuals who reported that they have ingested ivermectin every year during the past 5 years was 34.5% (95% CI: 30.8–38.4%), comparable between males (36.2%; 95% CI: 31.0–41.7%) and females (32.8%; 95% CI: 27.7–38.3%) (χ2 = 0.76, df = 1, P = 0.3833). A significant increase in the trend of compliance with ivermectin treatment was observed between the age groups (χ2 = 64.08, df = 3, P < 0.0001); 22.6% (95% CI: 16.3–30.4%) of participants aged 10–19 years (individuals < 10 years-old excluded), 20.4% (95% CI: 13.5–29.7%) of participants aged 20–34 years, 44.0% (95% CI: 35.1–53.4%) of participants aged 35–49 years, and 60.3% (95% CI: 53.1–67.1%) of participants aged ≥ 50 years declared having taken ivermectin tablets during the past 5 years.
The proportion of systematic non-compliers, that is those individuals who never ingested ivermectin tablets during the past 5 years, was 23.3% (95% CI: 19.9–27.1%), slightly higher in females (26.3%; 95% CI: 21.3–31.9%) than in males (20.4%; 95% CI: 15.9–25.7%) although statistically non-significant (χ2 = 2.5, df = 1, P = 0.1138). However, a significantly higher proportion of non-compliance with ivermectin treatment was observed between the age groups (χ2 = 24.59, df = 3, P < 0.0001). Participants aged < 34 years exhibited a higher proportion of non-compliance with ivermectin treatment compared to their older counterparts (χ2 = 64.08, df = 3, P < 0.0001). Overall, 31.6% (95% CI: 24.3–39.9%) of participants aged 10–19 years (participants < 10 years-old excluded), 36.6% (95% CI: 27.5–46.7%) of participants aged 20–34 years, 15.6% (95% CI: 10.0–23.6%) of participants aged 35–49 years-old, and 15.2% (95% CI: 10.7–21.1%) of participants aged ≥ 50 years declared that they have never swallowed ivermectin tablets during the past 5 years.
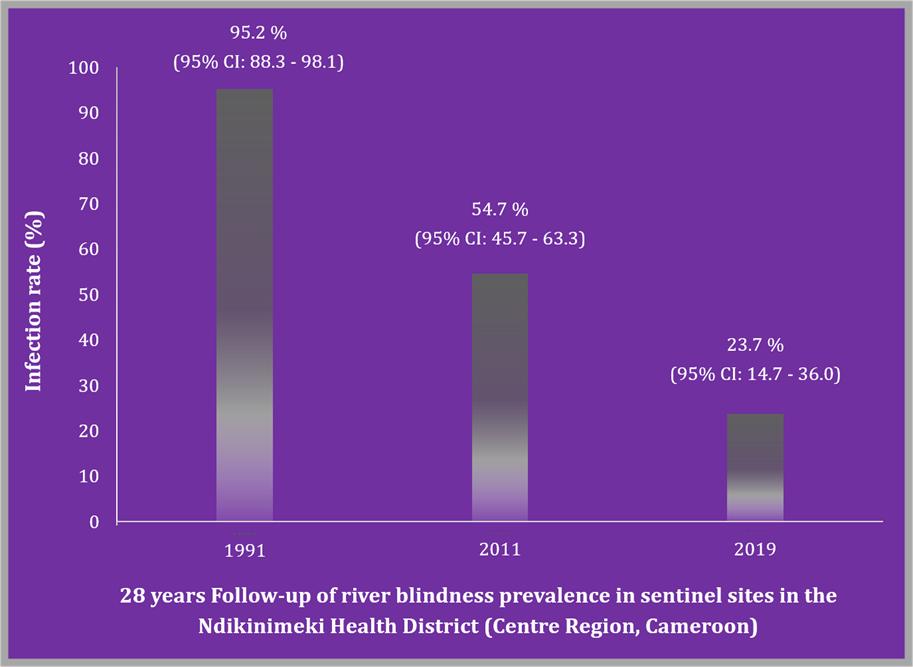
Thirty-year trend of onchocerciasis in the Boutourou Health Area
A significant decrease in the prevalence of onchocerciasis was observed, between the present findings (2019) and both baseline data (1991) (χ2 = 41.59, df = 1, P < 0.0001), and the first decade trend (2011) (χ2 = 15.25, df = 1, P < 0.0001) (Fig. 2).
{kind=link}