Our search identified 17,877 records and we assessed 54 full-text articles for exclusion by screening of titles, duplicates and abstracts. Twenty-two RCTs were included in the final analysis (PRISMA, Fig. 1). Twenty-one studies were published in English, and one French study was translated by a native speaking researcher (DM).
The 22 RCTs included a total of 3432 donors. Details of the included studies are shown in Table 1. Twenty-one RCTs were conducted in high income countries across Europe and North America, with one study conducted in Iran12, 13. Five RCTs evaluated systemic thyroid hormone therapy, four used systemic steroids and two studies used a combination of steroids and thyroid hormone. Further systemic treatments included albuterol, desmopressin, dopamine, protocolised fluid therapy, therapeutic hypothermia, naloxone, phentolamine, simvastatin, vitamin C or a protocolised ventilation strategy and were studied by one trial each. Almost one third (7/22) of all studies focused primarily on kidney transplantation and a further of eight studies were aimed at optimising donor factors in critical care. Four studies primarily studied lung transplantation, two studied liver transplantation and only one study was primarily aimed at heart transplantation.
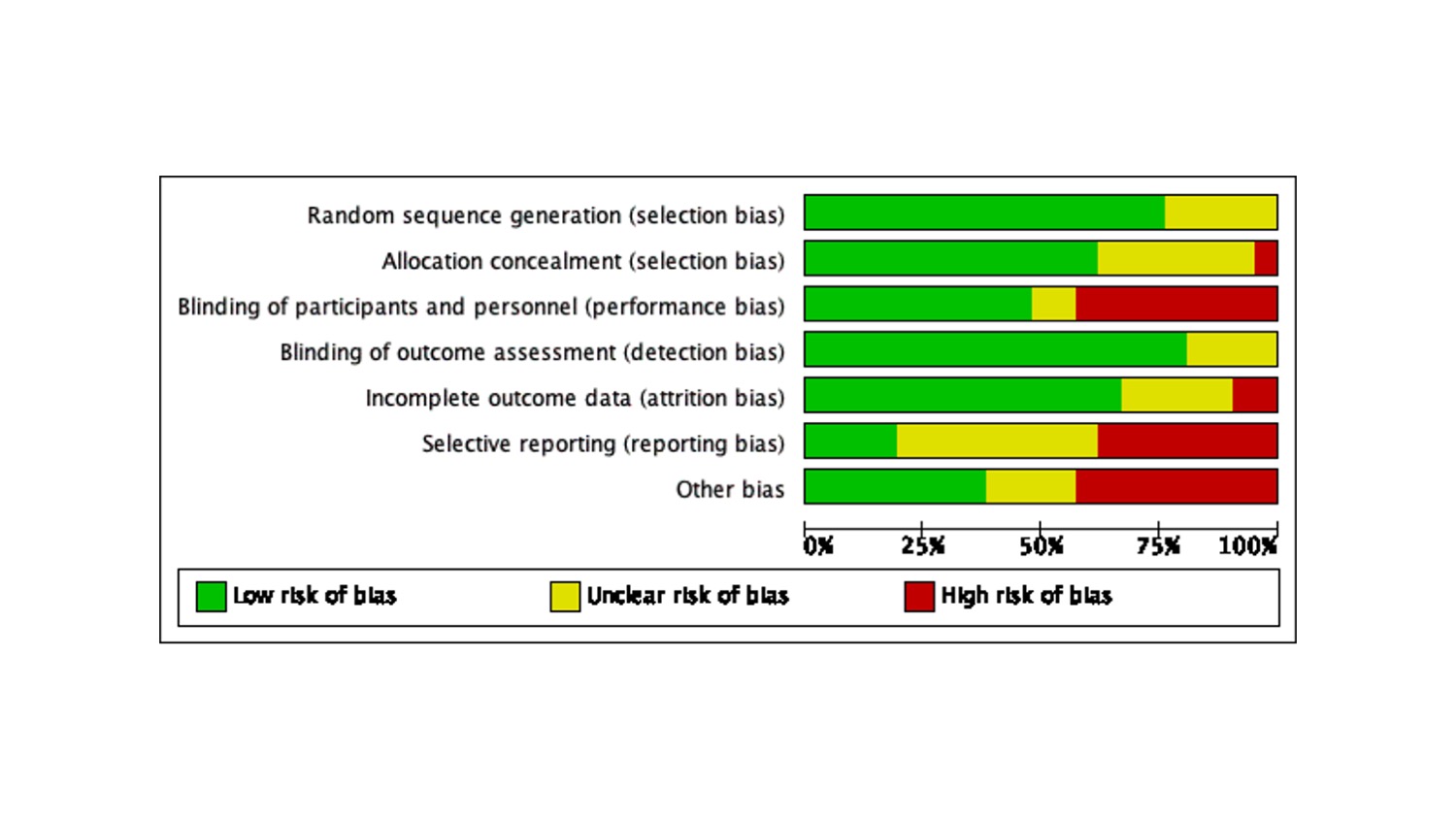
Risk of bias in included studies
All twenty two trials were assessed for risk of bias, with eight at high risk of bias (Fig 2). Only one trial was at low risk of bias14. Approximately a quarter of all studies were at high risk of reporting and performance bias. Further details of risk of bias assessments can be found in Additional file 3.
Synthesis of results
Multitude of reported outcomes across studies
Eight RCTs (36.3%) aimed to study the effects of the intervention on outcomes directly relevant during the donor management period in ICU. Amongst this group, named outcomes included: vasopressor/inotrope requirements, echocardiography parameters, number of transplanted organs, routine biochemical (e.g. thyroid function) or inflammatory (e.g. TNF-alpha) markers, or an assessment of haemodynamic stability. The remaining fourteen studies identified one transplanted organ as their main target, with the kidney (n=7) as the most studied graft, followed by lungs (n=4), liver (n=2) and heart (n=1). Amongst each of these, there was variation of the exact outcomes measured. Effects of treatments on pancreas were only studied in one trial15, whilst simultaneous kidney and pancreas and intestinal transplants were not studies in any of the trials.
Renal outcomes included post-transplant serum creatinine levels, presence of delayed graft function (DGF, defined as need for dialysis in first week post-transplant), primary non-function or biopsy-proved graft failure. Similar variability in organ outcomes was seen for studies focusing on the liver (post-transplant biochemical assessment versus record of graft function) or heart (echocardiogram assessment versus record of graft function) transplantation. All four studies of lung outcomes chose graft function before retrieval as their main outcome measure, whether by recording the number of lungs available for transplant or by reporting pre-specified outcomes such as final arterial blood gas or FiO2 prior to organ procurement14, 16–18. One study of lung transplants reported one year survival of recipients of other organs, although no record of graft function or survival was made16. The duration of follow up also significantly varied: ranging from reporting only outcomes before procurement (during duration of donor management) to trials with 5-year follow up, often published separately.
Outcomes by studied intervention
All included RCTs administered systemic treatment(s) to the randomised donor. Eleven studies studied the effects of steroids and/or thyroid hormone. The reported outcomes were grouped into outcomes affecting the major transplanted organs (kidney, liver, heart, lungs) or donor factors (such as factors haemodynamic stability or number of organs accepted for procurement). Figure 3 demonstrates that nearly all studies (21/22) of systemic treatments do not report outcome data across all the outcome domains. Only one study comparing ventilation strategies of the donor covered all outcome groups, albeit only reporting the recipient survival for each of the major transplanted organs14. Overall, the kidney or donor factor outcome groups were most often included, with each contributing to seven intervention types. DGF was the most common reported renal outcome (6/7 studies), whilst donor factors included a variety of different outcomes such as number of transplanted organs, inotrope or vasopressor requirement, left ventricular ejection fraction or cardiac index.
Outcomes by studied primary organ
Many of the selected outcomes depended on the primary target, e.g. kidney or physiological measurements in ICU. Studies focusing on kidney or heart transplantation were more likely to provide a more comprehensive assessment of other organs, as displayed in Figure 4. Early outcomes – defined as within 30 days of transplantation – more commonly reported surrogate outcomes such as changes in laboratory markers or echocardiographic function. Trials of interventions aimed at donor stability only rarely assessed organ specific function or outcomes – such as pre-transplant lung function, biochemical liver function assessment or mention of primary graft dysfunction for cardiac allografts. Furthermore, none of the donor stability RCTs assessed any long-term recipient or graft outcomes; therefore the long term effects of systemic treatment administered to nearly a quarter of all donors (23.3%, 800/3432) have not been collected by included trials. Organ-focused trials included long-term follow up of either one, three or five years of graft survival and between six months and three years of recipient survival as shown in Figure 5. Only one study reported the incidence of long term post-transplant complications relating to immunosuppression, such as post-transplant lymphoproliferative disease15. More specific measures of long term graft function after transplantation (such as creatinine or liver function tests) were only assessed in two studies19, 20. Organ specific rejection at 30 days and 3 months was studied in two trials aimed at the kidney21, 22. Rejection episodes within 6 or 3 years follow up were reported in both trials aimed at the liver20, 23. No studies reported on health-related quality of life in recipients of transplanted organs.
Exploratory analysis - Donor and recipient age, sex and ethnicity
In the UK, the NHS Blood and Transplant 2018-19 report describes the characteristics of 962 donors during that period: on average 51 +/- 16 years of age, mostly white (865/962, 90%) with an equal distribution of male (49%) and female (51%) donors. Only a minority of donors were reported as Asian (4%), Black (2%) or ‘other ethnicity’ (4%) 3. All included studies provide the age of the included donors, however the trial donor population is on average a decade younger than the average UK donor; In eight studies the average donor age was below 40 years and in 12 studies the average age was under 50 years. Donor sex information is available for n=2669 donors in total (20 studies) with 1596 (59.8%) male and 1073 (40.2%) female donors. Some individual studies, however, had groups more heavily skewed towards male donors12, 17, 24–26. Donor ethnicity was reported by three studies only16, 17, 27, with two further studies reporting the percentage of Afro-American donors in the two groups28, 29. The three studies which provide a breakdown of donor ethnicity describe a study population of between 60-80% white donors. Nine studies provide sex or age information for the recipients of the donated organs, whilst information on recipient ethnicity is not reported by any of the included trials.
{kind=link}