Study design and setting
This was a hospital-based, non-blinded, quasi-experimental study using a historical control group and an intervention group which was conducted at Amana, Mwananyamala and Temeke Hospitals, which are the three regional referral hospitals of Dar es Salaam, Tanzania. Each of these hospitals has a neonatal care unit admitting between 2800 and 4400 neonates every year.
Project implementation
A baseline survey of the historical control group was carried out from October 2018 to December 2018 using a structured questionnaire to collect demographic data of enrolled neonates and their mothers and to determine the time until critically ill neonates receive their first administration of mother’s milk, regain their birth weight and duration of hospital stay. At the same time adverse outcomes were monitored and documented.
While baseline data were being collected, a two-day workshop with the paediatricians responsible for the neonatal wards was conducted to develop locally adjusted standardized feeding guidelines for very sick and preterm neonates (see annex 1). A consensus was reached after review of the current literature and available feeding protocols from other centres. In a second workshop the local neonatal nursing staff created standard operating procedures (SOPs) on breastfeeding counselling, expressing breast milk, inserting a nasogastric tube (NGT) and feeding by cup or NGT.
After implementation of the new feeding guidelines and SOPs another period of 3 months data collection was conducted from February 2019 to April 2019 using the same data tool to obtain the corresponding data amongst the intervention group.
Study subjects
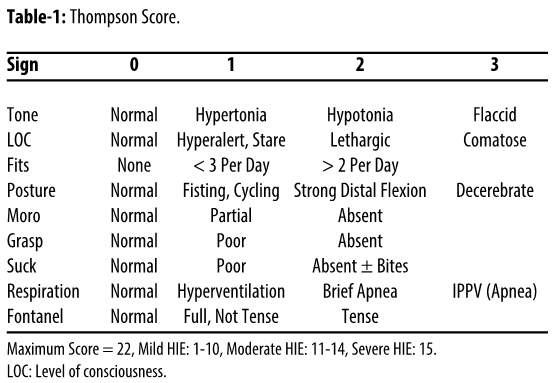
The study recruited neonates with VLBW and moderate to severe HIE admitted between October 2018 and April 2019. Neonates who were admitted > 24hours of life, born to HIV positive mothers who opted not to breastfeed, with features suggesting gastrointestinal malformations and those whose mothers declined consent, were excluded from the study. In a study done by Abdelmaaboud et al [24] in Quatar from 2009 to 2011 the proportion of NEC among neonates with delayed feeding was 12.9%. Using the power of 80%, at 95% confidence level with the assumption that introduction of early feeding will reduce the proportion of NEC by 80% (from 12.9–2.6%), the estimated sample size was 292. All eligible neonates were enrolled consecutively on admission until the sample size was reached.
Data collection methods and instruments
A pre-tested structured questionnaire was used to collect participant’s information including socio-demographic characteristics, feeding pattern, adverse events and neonatal outcomes. Dependent variables assessed were NEC as a primary outcome, neonatal mortality, time to regain birth weight and duration of hospital stay as secondary outcomes; while time to initiation of feeding was the independent variable.
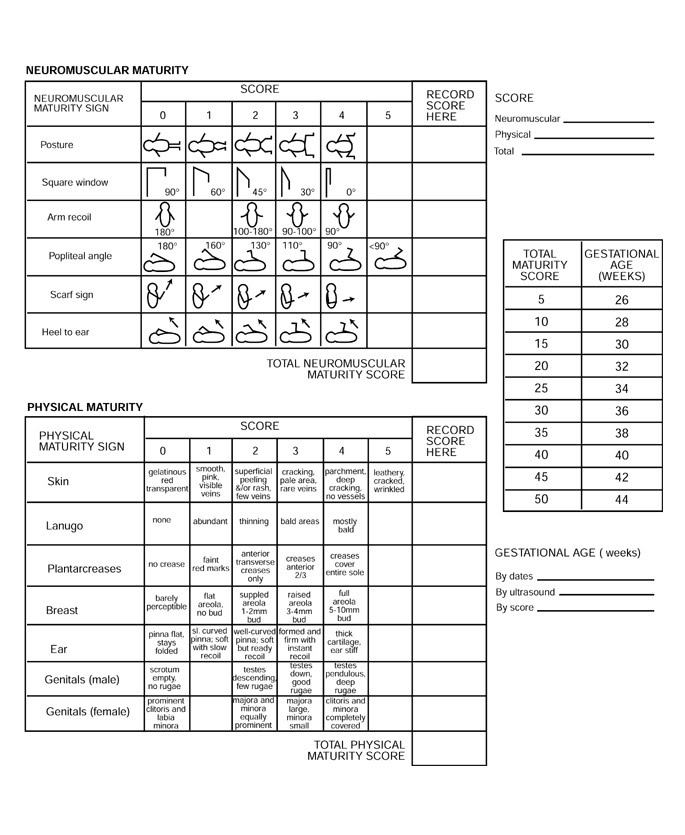
Study participants were enrolled during admission according to the inclusion criteria of birth weight 1000–1500 g for VLBW and Thompson HIE score > 10 for neonates with moderate to severe birth asphyxia. Body weight, gestational age (determined by Ballard score), HIE score and vital signs were recorded (see annex 2). Neonates in the historical control group started feeding after stabilization based on the decision of the attending paediatrician.
Study participants enrolled in the intervention group started early breast milk administration within 24 hours either by the means of OPC or MEN according to the newly implemented feeding guidelines as decided by the attending paediatrician. OPC was administered by giving 0.2 ml in each cheek using a 2 ml syringe. MEN was started with 10 ml/kg/day through NGT within the first 24hours and advanced at the rate of 20 ml/kg/day from the second day of life until reaching full enteral feeding of 150 ml/kg/day. Body weight was recorded every morning by trained research assistants.
If a neonate presented with abdominal distension, bilious vomiting and bloody diarrhea a plain abdominal x-ray was done to establish the occurrence of NEC which was diagnosed both clinically and radiologically using Bell's criteria whereby stage 2B was regarded as significant. A neonate with confirmed NEC was managed by the attending paediatrician following standard management guidelines.
During the intervention, participants’ safety was assessed through the monitoring for adverse events by a Data Safety and Monitoring Board (DSMB) comprised of independent reviewers. The DSMB consisted of one pediatrician, an epidemiologist and one biostatistics expert and met two weeks after data collection of the intervention group had started.
Data management and statistical analysis
Data was entered, cleaned and analyzed using SPSS version 20. It was an intention to treat analysis. The categorical variables NEC and mortality were presented using proportions. Continuous variables which were length of hospital stay and duration of regaining birth weight were presented using mean (standard deviation). Chi-square test or when appropriate Fisher’s exact test was used to compare statistical significance in outcomes. Odds ratio (OR) was used to determine association between independent variable (feeding type) and dependent variables. The results were considered of statistical significance when p-value was ≤ 0.05.
{kind=link}
{kind=link}