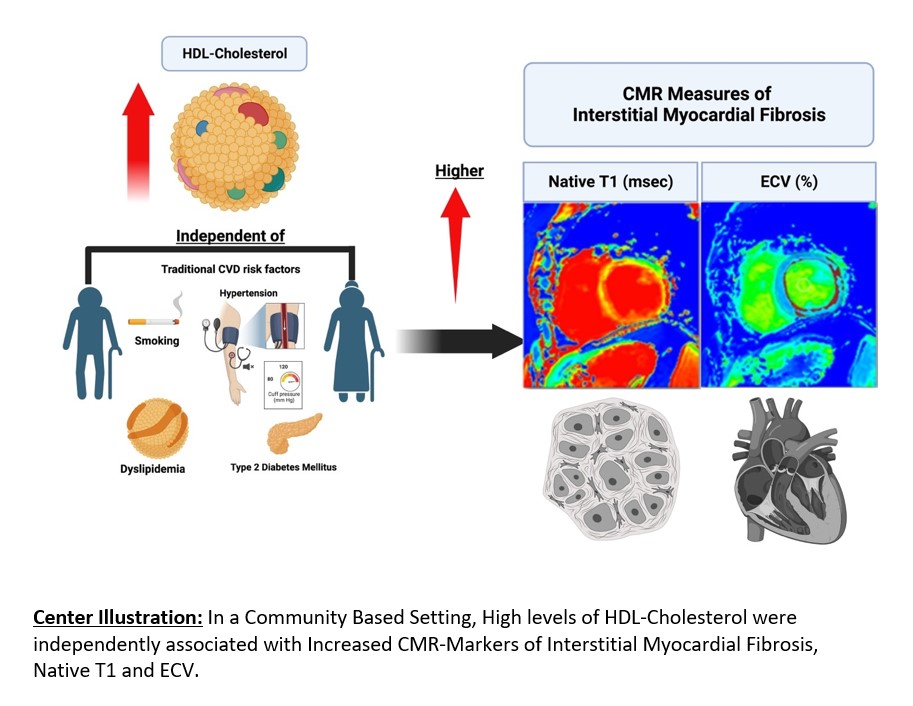
In our study, we evaluated the relationship between HDL-C levels with IMF, defined as an increase in native T1 time and ECV percentage, and the prevalence of myocardial scar in a population initially recruited without previous CV conditions. We now show that higher HDL-C levels were positively associated with greater ECV% and native T1 time. When stratifying HDL-C groups into low, reference, and high categories, our analysis further supported the assessment that high HDL-C is associated with subclinical fibrosis by CMR.
In a previous study, Rosmini et al. studied the effect of blood composition on T1 mapping in a cohort of 77 healthy individuals (6). They concluded that there was a positive correlation between HDL-C levels and native T1 time in the blood (7). Given that myocardial and blood T1 are closely correlated, our results support a similar conclusion, specifically that higher HDL-C was associated with increased myocardial native T1 and ECV on the population level. However, in our study, interestingly, native blood T1 time was not associated with HDL-C after adjusting for confounding variables, highlighting a potentially different mechanism between HDL and myocardial T1 analysis. Various conditions affect native T1 values of the myocardium, which will also be reflected in the ECV estimates. Longer native T1 times are associated with tissues where water molecules are less restricted, such as edema or inflammation, or in conditions associated with increased ECV, such as amyloidosis or fibrosis (13). On the other hand, lower values of T1 are seen in adipose tissues due to slower-moving protons and, thus, shorter T1 recovery time (13). One explanation for the observed results would be that elevated HDL-C levels affect the relaxation time of nearby photons and therefore affect the native T1 time, similar to the paramagnetic effect of iron in the hemoglobin on T1 relaxation time (14). Nevertheless, we observed that high HDL-C levels were associated with worse ECV and native T1 levels of 30% and 955 msec, respectively. Recent studies have shown that diffuse myocardial fibrosis evaluated by native T1 and ECV is associated with worse CVD prognosis, increased risk of congestive heart failure hospitalization, and all-cause mortality (9, 15–17). A previous analysis from the MESA found an ECV and native T1 cutoffs of 30% and 955 msec, respectively, were linked to worse cardiovascular events and mortality (9). Similar results were observed from the UK biobank that elevated levels of native T1 were associated with all-cause mortality, worse cardiovascular diseases, and events (12). However, further work will be needed to elucidate whether the association above reflects a causal contribution of HDL-C in the development of myocardial fibrosis or whether elevated HDL-C levels falsely elevate CMR markers of myocardial fibrosis by affecting T1 relaxation time (7).
To date, large randomized controlled trials that evaluated drugs such as niacin and treatment that inhibit the cholesterol ester transfer protein such as Tocertrapib have failed to show any signs of efficacy in increasing HDL-C in preventing cardiovascular events (18–20). Moreover, there is growing evidence in the literature suggesting that elevated HDL-C levels may not offer cardiac protection as previously thought (21). Several large cohorts found an increased risk of cardiovascular disease with high levels of HDL-C, similar to low levels of HDL-C (21). A recent study that included two prospective cohorts, the UK and Emory Cardiovascular Biobank, found that compared with those with 40 to 60 mg/dL HDL-C levels, individuals from the Emory Cardiovascular Biobank with very high HDL-C levels (> 80 mg/dL) had a higher risk of all-cause death (1.96 HR, 95% CI 1.42–2.71, P < 0.001) and cardiovascular death (1.71 HR, 95% CI 1.09–2.68, P = 0.02) after adjusting for confounding factors. Similar results were observed in the UK biobank and after adjustment of HDL-C genetic risk scores (4). In another prospective cohort of more than 100,000 participants from the Copenhagen City Heart Study and the Copenhagen General Population Study in Denmark, there was a U-shaped relationship between HDL-C and risk of all-cause mortality, with the high risk being found among low and very high levels of HDL-C (5). This association was similar in both men and women. Our research findings suggest a potential link between both lower and higher levels of HDL-C and an increased prevalence of myocardial scar. Specifically, individuals with lower HDL-C levels exhibited a slightly elevated risk (OR: 1.1, 95% CI: 0.58–2.21), while those with higher HDL-C levels demonstrated a moderately increased risk (OR: 1.5, 95% CI: 0.81–2.89), compared to those with normal HDL-C levels. However, it's important to note that these associations did not reach statistical significance in our analysis.
Our current study found that increased HDL-C was associated with markers of IMF irrespective of sex. However, when stratified by sex, we found that the association was more evident in men; however, an increase in HDL-C was also associated with a significant increase in native T1 in women. Given that women have higher levels of HDL-C, this could be one of the reasons underlying the baseline elevation of IMF markers compared with men (4, 10).
Another potential theory behind the increase in markers of IMF among those with high HDL-C includes a “loss of function” or “dysfunction” of HDL-C (21). HDL dysfunction has been found to decrease the ability to promote cholesterol removal from macrophages, prevent LDL oxidation, and control apoptosis, nitric oxide production, monocyte chemotactic protein-1, and vascular cell adhesion molecule expression in endothelial cells. Patients with altered HDL were found to have suppressed nitric oxide production through interaction with LOX-1, TLR2, and TLR4 receptors (21). This leads to the phosphorylation of inhibitory sites in eNOS instead of activating sites (22).
Other causes were linked to the inflammatory markers of the lymphocyte activation gene- 3 (LAG-3). Prospective cohorts have found that a decrease in plasma LAG3 protein was one of the causes of the elevation of HDL-C, which was then associated with an increased risk of coronary artery disease (23). We recently reported that in MESA and the Framingham Heart Study (Offspring cohort) the following plasma proteins were positively associated with LAG3 and HDL-C: IGF1R [insulin-like growth factor 1 receptor], LRIG3 [leucine-rich repeats and immunoglobulin-like domains 3], and DCTPP1 [DCTP pyrophosphastase 1] whereas GFRA1 [glial cell line-derived neurotrophic factor family receptor alpha 1] was inversely associated with HDL-C (24). Abdellatif et al. examined the role of cardiac IGF1R signaling in an aging model in male mice (25). These investigators found that young male mice with increased IGF1R signaling exhibited superior cardiac function but this rapidly deteriorated with aging, with decreased autophagic flux and impaired oxidative phosphorylation. For LRIG3, there has been one report of impaired cardiac function and low HDL-C in Lrig3-/- mice (26). For DCTPP1 and GFRA1, a PubMed search did not identify any publications linking either protein with HDL-C, myocardial fibrosis, or myocardial scarring. Other possibilities include genetic variants associated with reduced expression of scavenger receptor class B type I protein (SR-BI), which leads to elevated HDL-C and MI risk (21, 27). Muthuramu et al showed that expressing hepatic SR-BI in the liver significantly reduced cardiac dysfunction in Scarb1-/- mice, a mouse model well-known for high HDL-C, accelerated atherosclerosis and coronary artery rupture (27).
Limitations
Our study includes several limitations. First, this was a cross-sectional study design; therefore, a causal relationship between HDL-C and CMR measures of myocardial fibrosis cannot be determined. In addition, some factors might affect measures of interstitial fibrosis, such as iron and albumin were not available. It is not clear whether the elevated ECV and native T1 result from an increase in HDL-C or HDL -C alters native T1 time and ECV percentage in a way similar to iron and hematocrit through changes in blood T1. Nevertheless, we showed that pathologically elevated levels of ECV and native T1 were associated with an increase in HDL-C. Even though interstitial fibrosis is the most common determinant of altered T1 indices in this community population, CMR T1 mapping indices are not specific to myocardial fibrosis. A build-up of the extracellular matrix usually occurs because of increased interstitial fibrosis but may also result from edema, hypertrophy, or other cardiac infiltrative disorders. Lastly, those who declined a CMR contrast agent or were not eligible for it could have been systematically healthier than those who were eligible. Thus, temporal or selection bias could not be ruled out. However, even after excluding participants with cardiovascular events such as MI or congestive heart failure, there was a positive relationship between HDL-C and increased CMR markers of interstitial myocardial fibrosis. Nevertheless, CMR T1 mapping and LGE are reliable and noninvasive methods for evaluating myocardial fibrosis with native T1, requiring no contrast injections. This makes it accessible to patients with impaired renal function.
{kind=link}